Connecting people with information needed to live their best possible lives.
Chronologic by year:
- Emergency Use Authorizations in a Post-Emergency World

According to the U.S. Department of Health and Human Services (HHS), the COVID-19 Public Health Emergency will expire in May, but Emergency Use Authorizations and liability protection will continue after the emergency ends.
Early in the pandemic, we were told that Emergency Use Authorizations were necessary to make unlicensed, unapproved tests, vaccines, and treatments available during an emergency. On January 31, 2020, the Health and Human Services Secretary declared the COVID-19 pandemic a public health emergency, paving the way for these products. The secretary even invoked the liability protection of the PREP Act to encourage manufacturing of countermeasures. Soon, the FDA began issuing Emergency Use Authorization letters which close with a notice that the authorization will terminate when the emergency is over.
Last month, the HHS secretary signaled his intention to end the emergency on May 11, 2023. At the same time, the secretary assured us that Emergency Use Authorizations will not be affected. According to the statement, “Existing EUAs for COVID-19 products will remain in effect under Section 564 of the Federal Food, Drug, and Cosmetic Act, and the agency may continue to issue new EUAs going forward when criteria for issuance are met.”
The Federal Food, Drug, and Cosmetic Act was amended several times by the Consolidated Appropriations Act, 2023 (see page 1339, for example). Did these amendments give FDA authority to issue EUAs without an emergency? I cannot tell you because, frankly, I get lost in the language. HHS claims its authority for EUAs in the absence of an emergency declaration dates back a decade, to the Pandemic and All-Hazards Preparedness Reauthorization Act of 2013. Regardless, the intention is clear: EUAs will continue after the emergency is lifted.
And what will become of those PREP Act liability protections? According to HHS, these will also continue, but only for a select group of manufacturers:
Currently, the amended PREP Act declaration provides liability immunity to manufacturers, distributors, public and private organizations conducting countermeasure programs, and providers for COVID-19 countermeasure activities related to a USG [United States Government] agreement (e.g., manufacturing, distribution, or administration of the countermeasures subject to a federal contract, provider agreement, or memorandum of understanding). That coverage will not be affected by the end of the PHE. However, PREP Act liability protections for countermeasure activities that are not related to any USG agreement (e.g., products entirely in the commercial sector or solely a state or local activity) will end unless another federal, state, or local emergency declaration is in place for area where countermeasures are administered. HHS is currently reviewing whether to continue to provide this coverage going forward.
Fact Sheet: COVID-19 Public Health Emergency Transition Roadmap, February 9, 2023Manufacturers of EUA products that have an agreement with the US Government will continue to have liability protection. Other manufacturers will not. Collusion between the federal government and big businesses like this asymmetric post-emergency liability protection is the very definition of fascism.
If Emergency-Use-Authorizations without an emergency seem illogical to you, you are not alone. Even members of congress have assumed that EUAs will end with the emergency declaration.
This is not just an assault on language and logic. It is an assault on liberty.
The emergency declaration will end soon, but the emergency power-grab will continue indefinitely.
- Shouldna Listened to That Doc
The American Medical Association (AMA) urges physicians to promote COVID-19 vaccines and bivalent boosters. The AMA even supplies members with social media talking points and strategies to deal with vaccine detractors. It is not the first time that my profession has endorsed a product that may be hazardous to your health.

For most of the twentieth century, the AMA turned a blind eye toward the dangers of tobacco use. During the 1930s, 40s and 50s, tobacco companies paid handsomely to advertise cigarettes in AMA’s journal, JAMA. In a 1948 editorial minimizing the ill effects of smoking and justifying tobacco advertising in its publications, JAMA noted that “cigarette business is a tremendous business,” as if the size of the bottom line can mitigate a conflict for an organization founded for the “betterment of public health.”
The connection between smoking and lung cancer was recognized early in the century. At the same time, the AMA became increasingly dependent on money generated by tobacco sales. Tobacco companies sponsored meetings of medical societies, setting up their booths alongside exhibitions of the latest medical treatments. Free cartons were distributed at physician meetings. Cigarette makers even paid for publication of pseudoscientific reports claiming the health benefits of their products.

Doctors who opposed smoking faced ridicule from their colleagues. Dr. Alton Ochsner, a renowned surgeon and sentinel voice warning of the dangers of tobacco, began publishing on the connection between smoking and lung cancer in the early 1940s. His 1954 book Smoking and Cancer: A Doctor’s Report was negatively reviewed in prominent medical journals, characterized as a medieval model of logic that belongs in the nonscience section of a library. Prior to his appearance on Meet the Press, Dr. Ochsner was told he could not discuss the relationship between smoking and lung cancer on air.
Yet the mounting evidence was hard to ignore. In 1954, JAMA stopped accepting cigarette advertisements and published an editorial rebuking tobacco company advertising practices. But fives years later, a JAMA editorial was still skeptical of the evidence linking smoking to cancer, and a 1961 Nebraska State Medical Journal editorial dismissed the evidence as merely “statistical.” Tobacco companies continued to sponsor state medical meetings as late as 1969. By then most people were aware of the dangers of smoking.
In 1964, the Surgeon General concluded that cigarette smoking causes lung cancer and other life-limiting health conditions. The next year, a warning label was required on packages of cigarettes. By 1971, the government banned cigarette advertisements on television and radio. Instead of taking the lead against an obvious threat to public health, the AMA asked for time and money to study the effects of tobacco.

Between 1964 and 1976, the AMA received more than $20 million from the tobacco industry to fund research. Instead of using the money for smoking cessation programs, many of the funded studies focused on ways to make a safer cigarette. To keep money flowing into its Education and Research Foundation the AMA delayed, stating in a confidential 1971 report that, “AMA is not prepared to make any statement regarding termination of the smoking-health research program.” The report went on to complain that tobacco companies are “in arrears on 1970 contributions.” The dependency on tobacco money created a political alliance between doctors and cigarette makers as their lobbyists joined forces in Washington.
The delay benefitted tobacco sales and maintained the AMA’s “research” payments, but it angered Dr. Ochsner, who accused the AMA of being derelict. The AMA called Dr. Ochsner’s position “extreme.” However, name-calling could not stall the inevitable conclusion any longer. In 1978 the AMA finally agreed with what most people had already realized: smoking causes lung cancer, and many other health problems. The romance with big tobacco was over.
Or was it?
As late as 1982, JAMA publications were warned to steer clear of “politically sensitive” topics like tobacco use. After most of a century of being on the tobacco dole, the AMA could not make a clean break. The AMA portfolio contained investments in tobacco companies until the late 1990s.
In 1998, the tobacco industry settled lawsuits filed by state governments with a massive Master Settlement Agreement. In exchange for perpetual annual payments and tight regulatory control, the tobacco industry could continue to sell its products protected from future lawsuits brought by participating states and jurisdictions.
But who really benefitted from the Tobacco Settlement? Only 2.6% of the money has been used for smoking prevention and cessation programs. Some states have used the tobacco money to fill budget gaps. South Carolina gave money to tobacco farmers affected by a drop in prices. Altria Group, a global tobacco company, is on the US News 10 best-performing stocks list. Altria, Phillip Morris, and British American Tobacco have all grown annual dividends consecutively since the settlement. According to Dr. Ed Anselm, “The most addictive thing about tobacco is money.”
Tobacco use remains the number one preventable cause of death in the United States. In the first fifty years after the Surgeon General’s 1964 report, more than 20 million Americans died of smoking. How many of these deaths would have been prevented if doctors had not been conflicted by financial entanglements with the tobacco industry?
Money blinds objectivity. When money drives decisions, controverting evidence is ignored, dissenting voices are ridiculed, open debate is suppressed, talking points are distributed, conclusions are delayed, and people die from a product with liability protection.

The New York State Journal of Medicine published a retrospective of tobacco’s relationship to medicine in its December 1983 issue. Flipping through the pages is enlightening. Surrounding the articles describing the greed and politics of big tobacco are advertisements from medicine’s new love—big pharma. Doctors have exchanged one bedfellow for another.
By endorsing irrelevant COVID-19 vaccines and poorly tested bivalent boosters, the AMA is pushing a product without concern for its potential negative health effects. Like before, the medical profession lags behind public opinion. According to recent Rassumsen Reports, 7% of vaccinated individuals report a major side effect, and nearly half of Americans believe that COVID-19 vaccines have caused unexplained deaths, about the same proportion who believed that smoking caused cancer in the 1960s while the AMA was studying the issue.
A conflicted profession cannot honestly evaluate data. Nowadays, the pharmaceutical business is a tremendous business. An organization benefitting from a product’s sales cannot be trusted to evaluate that product.
If doctors could not recognize the health dangers of tobacco for most of the last century, why should we believe them when they say novel vaccines are safe and effective?
Additional Resources:
- Vaccination Does Not Prevent Long COVID

Infections by SARS-CoV-2 can cause acute COVID-19 which may last up to four weeks. Post COVID Conditions, also known as Long COVID, are health consequences that persist or develop more than four weeks (or twelve weeks, according to WHO) after infection. Individuals who have had acute COVID-19 are at risk for Long COVID.
According to government health agencies, Long COVID prevention is another reason to get vaccinated. Without offering any evidence, or even a plausible mechanism for why it might be so, the CDC says that “people who did not get a COVID-19 vaccine” are more likely to develop Long COVID. Health+ Long COVID, a report sponsored by HHS and released last month, contains the recommendation to “promote vaccination as a preventative measure for Long COVID.” NIH even encourages unvaccinated people to get vaccinated after recovering from COVID-19 because it “may prevent Long COVID.” But there are good reasons to doubt that any of this is true.
Long COVID can follow mild or asymptomatic infections by SARS-CoV-2. Although there may be more than one pathway to Long COVID, autoimmunity is responsible for some, if not most, cases of Long COVID. The intensity of the initial disease does not matter. Mild or asymptomatic infections can stimulate the autoantibodies that cause Long COVID. Even if you believe that vaccination reduces severity of COVID-19—I am not saying you should—there is still no reason to believe that vaccination can prevent Long COVID.
Recent studies back this up. According to an article published in Nature last month, vaccination status does not modify the risk of Long COVID. Instead, Long COVID correlates to the number of SARS-CoV-2 infections a person has, regardless of vaccination status. Even though vaccination cannot prevent Long COVID, it may make it worse.
Think about how autoimmunity causes Long COVID. Once the immune system is stimulated to recognize the spike protein of SARS-CoV-2, the immune system may attack the body’s own cells. Whether by an accident of nature or by design, antibodies to spike protein cause autoimmune disease in some people. It does not matter whether the antibodies are formed in response to vaccine or natural infection, the effect is the same. Vaccination injuries can look like Long COVID.
Dr. Marivic Villa, a Florida pulmonologist who has treated thousands of COVID patients in The Villages, agrees. According to a recent publication, Dr. Villa says, “The signs and symptoms profile and clinical presentation of long-haulers from moderate to severe natural COVID infection, and individuals vaccinated three to four times, are almost indistinguishable from one another.” The formation of autoantibodies by either natural infection or vaccination connects Long COVID to vaccine injuries, consistent with Dr. Villa’s observation. She concludes, “Halting this vaccination is the highest emergency!”
Long COVID has White House attention. This focus seems timed to perpetuate the emergency, just like the government distribution of free tests earlier this year. These substandard tests, purchased by the government and mailed to anyone with a U.S. address, were bad laboratory medicine, saved no lives, and have not been missed since funding ran out. But the program stirred up COVID activity, keeping the crisis going. And it enriched test suppliers.
Similarly, attention to Long COVID is a pretext to extend the emergency powers of the executive branch by combining a tragic reality with bad medicine, unsupported by honest science. And it enriches vaccine manufacturers.
Every case of COVID-19, every SADS death, every victim of Long COVID, and every individual injured by vaccine is a life lost or damaged by the tragedy of the pandemic. Long COVID cannot become just another excuse to promote vaccine.
- The Never-Ending Emergency

I have been quiet lately, not wanting to add to COVID saturation. The issues of the pandemic are well known—viral origin, vaccine safety, early treatment, repurposed therapeutics, pharma windfalls. The word is out, everyone has an opinion, and most have dug in. One way or another, we have all learned to cope with a virus that is here to stay.
From this state of uneasy equilibrium, I must ask why we are still in a declared state of COVID-19 emergency. Maybe we need to start with the meaning of emergency.
Many years ago, a good friend of mine was pulled over. The officer invited him to the back of the car, put him in handcuffs, and hauled him to jail. A check of his license plates revealed a warrant for his arrest, except it was a mistake. My friend had done nothing wrong. A clerical error associated his plate number with someone else’s warrant. Nonetheless, he found himself in the county jail. On the wall of the cell was a dirty red button, and under the button was a sign, “Press for emergency.” He felt entitled to press the button.
“What is your emergency?” Came the voice out of the speaker.
“Well, you see, I shouldn’t be here…” Click.
The speaker went silent, so he pressed the button again.
“What is your emergency?”
“I believe there must be some mistak…” Click. He pressed the button again.
“What is your emergency?”
“I need to make a phone ca…” Click. By now, he realized that his situation, however unpleasant, inconvenient, and unjust, did not constitute an emergency, so he prepared to spend the night alone in the cell, which he did. The next morning the mistake was realized, and he was released, unceremoniously, with barely an apology, and no compensation for his 17-hour ordeal.
COVID-19 is like this. It is unpleasant, inconvenient, and even unjust, but it not an emergency. At least not anymore.
This view has gained broad consensus across the political spectrum. Most states have ended emergency measures, and California will join that list soon. With a nearly veto-proof bipartisan majority, the US Senate voted to end the emergency earlier this month. Even President Biden has said the pandemic is over. Yet his administration promises to veto the Senate bill if passed and to extend the emergency declaration again next year. All for an emergency that is as real as the tooth fairy.
And why not? The emergency declaration has been the tooth fairy for many.
The COVID emergency is a bonanza for manufacturers of counter-pandemic measures—vaccines, tests, and drugs among them. Not only does it give them an endless market for their products, but bypassing FDA approval saves them millions. And they also receive liability protection for any product manufactured under Emergency Use Authorization. No wonder the healthcare manufacturing sector never wants the emergency to end.
The American Hospital Association also lobbies for continuing the emergency, and for similar reasons. Hospitals get a 20% bonus for treating COVID patients. CMS relaxed regulatory standards during the emergency. And there is funding for “building vaccine confidence.” But none of this would happen without the consent of government.
The executive branch of government has used COVID-19 as excuse for a power-grab. During a crisis, citizens—including members of congress—are willing to temporarily cede power to the executive in exchange for steady leadership through the emergency. The trouble is that the executive branch jealously clutches power gained during turbulent times once calm is restored. History backs me up. World War I gave us the Espionage Act of 1917. September 11 gave us the Patriot Act of 2001. And the COVID Pandemic gave us the Declaration Under the PREP Act for Medical Countermeasures Against COVID-19.
Last month, right on cue, Xavier Becerra renewed the emergency for the twelfth straight quarter, extending the government’s emergency powers into 2023. Many of these “emergency” measures are difficult to connect to the pandemic. For example, the CDC issued an eviction moratorium that had to be struck down by the Supreme Court. HHS approved use of Medicaid funds to pay for food and housing in Massachusetts and Oregon. The emergency is even the basis for President Biden’s proposal to forgive student loans. The emergency has allowed the administration to short-circuit the checks and balances in normal policymaking processes, giving it autocratic power.
The emergency has become an institution. Many are dependent on emergency measures, so there will be pain when the emergency ends. But delay will only increase the suffering we must endure later.
The emergency is over. Policies must stand on their own merits. Normal processes must return.
- Immunizations for Vaccinations

Last week, CDC published an interim COVID-19 vaccination schedule that recommends unapproved COVID-19 vaccines for routine administration to children less than twelve years of age. This is the first time CDC has placed an unapproved vaccine on the childhood vaccination schedule, permanently transferring liability for these vaccines from the manufacturer to American taxpayers, even after the emergency ends. Only Congress can change this now.
We knew this was coming. The PREP Act Declaration issued by the Secretary of HSS more than two years ago granted immunity “from suit and liability under Federal and State law with respect to all claims for loss caused by, arising out of, relating to, or resulting from the administration or use of a covered countermeasure” while the nation is under the COVID-19 emergency declaration. “Countermeasures” include vaccines.
PREP Act immunity is not permanent. When the emergency declaration is finally lifted, continued use of COVID-19 vaccines will expose the vaccine manufacturers to liability unless it becomes a “covered vaccine” under the National Vaccine Injury Compensation Program.
What is a covered vaccine?
For a vaccine to be covered, the Centers for Disease Control and Prevention (CDC) must recommend the category of vaccine for routine administration to children or pregnant women.
Those where not my words; they come directly from the HRSA website. Once covered, the vaccine is protected for all recipients, not just children and pregnant women. By recommending COVID-19 vaccines for children, the CDC transferred all associated product liability to the American taxpayer.
This action is an assault on many levels, but I want to focus on only one. The recommendation applies to an unlicensed product. No matter your opinion of FDA’s approval and licensing process, the process should be completed before a product is recommended for routine use. An emergency use authorization does not apply to non-emergent administration.
COVID-19 vaccines are not approved for anyone younger than 12 years of age. Furthermore, approved COVID-19 vaccines remain unavailable to Americans of any age—although that will probably change now that permanent immunity has been secured. A vaccine that is not approved for children should not be recommended for children, and it has never happened before. This is the first time that the recommendation for routine administration has preceded FDA approval.
FDA approval is a slow and laborious process with many critics. Despite decades of attempts at acceleration, at the pandemic’s outset the FDA’s process was seen as a liability that put Americans at greater risk than citizens of other nations. The fear that the FDA would slow down an effective pandemic response led to the emergency declaration by HHS and the use of Emergency Use Authorizations to bring new countermeasures to market. Although careful, meticulous approvals can be painstaking, rapid approvals compromise safety. I did not take an oath to eliminate frustration; I took an oath to do no harm.
But what harm is there in vaccine? Surely vaccines are the most benevolent of therapies, protecting against dread diseases while rarely causing harm.
This thinking is an example of association fallacy. A risk-benefit analysis that favors some vaccines is not a favorable risk-benefit calculation for all vaccines. Each vaccine must be carefully evaluated on its own merits. The slow, methodical FDA approval process meets that standard. Or at least I thought so.
FDA’s approval process has let us down, plenty of times. Think of television commercials promising large litigation settlements to victims of injury by various drugs. There will be no such advertisements for COVID-19 vaccine injuries since these vaccines have immunity under the law. Unless the law changes.
Congress has the power to change law, and Congress has the duty to change bad laws.
Although Congress did not directly grant liability protection to COVID-19 vaccine manufacturers, by passing the National Childhood Vaccine Injury Act of 1986, the 99th Congress created a loophole that gave the CDC power to shelter COVID-19 vaccine manufacturers from liability, setting the stage for what happened last week.
CDC’s actions are unprecedented. Recommending an unapproved vaccine for children is reckless. Transferring product liability risk from manufacturers to taxpayers is corrupt. Congress owns this. Congress can change this.
The election for the 118th Congress is only days away, and early voting has already begun. Please keep this in mind as you consider your vote.
- The Vaccine Is a Virus

mRNA Vaccine Lipid Nanoparticle A virus is a sequence of genetic code wrapped in an envelope. Viruses are classified by their envelope and genetic code configurations. Since they do not possess independent means of reproduction, viruses are not technically alive, yet they yield to the primal force of life—the urge to propagate their genes. To do this, each virus seeks a host, hijacking its means of reproduction to pump out as many copies of the virus as possible. Each copy seeks its own host to infect, and the cycle repeats. In this way, the virus and its genes live without being alive.
An mRNA vaccine is a sequence of genetic code wrapped in an envelope. The genetic code is messenger RNA and the envelope is a lipid nanoparticle, but that does not change the similarity to a virus. Like a virus, each mRNA vaccine particle infects a host cell, hijacks the cell’s means of production, and pumps out copies of the encoded spike protein.
Both virus and vaccine introduce spike protein into the body. When virus enters through the nose and upper airways, the spike protein on the virus causes an immune response and spike antibodies are formed. A successful immune response clears the virus, but the immune memory lingers, spike antibodies and all. Inoculation by mRNA vaccine is also an infection, except this infection occurs in the arm.
We were told—and I wrote in this blog—that vaccine mRNA stays in the cells of the arm muscle and is broken down quickly, but that is not true. Studies published this year have demonstrated vaccine mRNA in breast milk, blood, lymph nodes, liver, and skin. Unlike spike protein from a mild infection, vaccine induced spike protein can be detected in blood up to four months after vaccination; from there, it can distribute widely throughout the body. Clearly, the mRNA does not stay in the arm and is not broken down quickly. Compared to natural infection, genetic COVID-19 vaccines are more likely to spread spike protein throughout the body.
This wide distribution of vaccine is significant. Every cell that ingests a lipid nanoparticle will express spike protein, marking the cell as an immune target. As a result, the cell will die. This process is a direct mechanism for adverse effects like vaccine-induced myocarditis. When a heart muscle cell absorbs vaccine, the spike proteins generated incite inflammation that kills the cell. If this happens to enough heart cells, the person will die—suddenly and unexpectedly.
Yet this mechanism may not explain all the adverse effects of vaccines. Serious conditions such as acute myocardial infarction, Bell’s palsy, cerebral venous sinus thrombosis, Guillain–Barré syndrome, myocarditis, pericarditis, pulmonary embolism, stroke, thrombosis with thrombocytopenia syndrome, appendicitis, herpes zoster reactivation, neurological complications, autoimmune hepatitis, and autoimmune peripheral neuropathies have been reported.
Since these conditions have also been observed after SARS-CoV-2 infection, a common autoimmune pathway is proposed. Whether introduced by virus or vaccine, spike protein shares features with molecules naturally found in the body. There are enough similarities that antibodies to spike protein may cause disease. The antibodies that remain after infection or inoculation are unable to distinguish between the harmless molecules of the body and viral spike protein. The result is an attack on one or more parts of the body by the body’s own immune system.
SARS-CoV-2 virus and mRNA COVID-19 vaccines share structural features and pathogenic effects. Both consist of genetic material within a lipid envelope. Both introduce spike protein to the body, and both stimulate antibodies against spike proteins and their lookalikes, which may damage one or more organs. The adverse effects of vaccine can look like long COVID.
The vaccine is a virus, with one important difference. The virus, you catch. The vaccine, you take.
- A Life Well Lived
Next to my wife and family, medicine is my life. But can a life in medicine be a life well lived?
First some definitions. To me, the difference between life and death is consciousness, and consciousness is awareness and activity. Awareness and activity require memory of the past and projection into the future. Maybe you disagree with these definitions, but stick with me for a few minutes.
The arrow of time moves in one direction only. The past is unchangeable, and the future is unknowable. The point at which future turns into past is now, and now is where experience happens. Experiences are the elementary particles of life.
There are many kinds of experiences. Some experiences are trivial, others are profound, and many are mutually exclusive. Every life is filled with experiences, but which experiences make a life well lived?
Self-awareness—knowing who you are—guides the selection of experiences that separate a life without meaning from a life well lived. But you may not be who you think you are. For example, you are not the sum of your talents. A virtuoso is not just a musician—that would be sad, just as sad as a talented doctor who is only a doctor. You are not any degree, profession, certification, achievement, success, or accomplishment you may have earned. These are things you have done, not who you are.
You are not your personality. Personality describes a style comfortably worn, like a pair of jeans or a favorite coat. You are much more than what you wear. You are the core that your personality covers, the essence that is served by your skills and talents. You are who you are wired to be.
A life well lived is a life filled with experiences that resonate with who you are.
Filling your life with experiences that match your essence puts you in flow, the state of complete immersion in an activity, where time is distorted, and joy is maximized. This works regardless of your occupation. I spend a lot of my time at work in flow.
I share the talents of many of my colleagues—determination, persistence, stamina, pragmatism, independence, and the ability to think logically—talents suited to medicine. My Meyers-Briggs type is ENTJ, which makes me a bit atypical for a pathologist. My education and training took more than half the life I have lived so far. But none of these are who I am.
I am wired to help people have a better future. Many people are wired the same way, and it sounds grander than it is. I am wired for better, not for perfection. My scope is people in my reach, not every person on earth. This is who I am, whether I am a doctor, a neighbor, a husband, or a father.

I earn my living as a pathologist, and my professional life is filled with experiences that connect people with information they need to have a better future. My job takes me into worlds most people do not know exist. When I look in my microscope, I see colors, shapes, and beauty. I see heroes and villains, tension and resolution, turmoil and peace. In these fanciful places, I find what people need. I dig it out, distill it, package it, and deliver it, connecting people to it. It is satisfying work because it is consistent with how I am wired. Many times, I am arming someone on a hero’s journey, standing at the edge of the abyss. Many times, I am helping my colleagues do what they are wired to do. But my profession does not determine the value of my life; doing my job in a way that resonates with who I am is what makes my life fulfilling.
It is possible to have a life well lived in medicine, but not because it is a life in medicine. A life well lived in medicine is like any other life well lived. It is a life filled with experiences selected to match the core of being. Every life contains the promise of a life well lived. My potential for a life well lived will continue even if my life in medicine ended today.
But there is a flip side, a warning especially for those who share my profession.
A life filled with experiences that conflict with being is a life of dissatisfaction and dysfunction. Joy is lost. Boredom, anxiety, or both creep in. This is where burnout happens, and it happens in medicine—a lot.
When physicians focus on the past or the future instead of the patient in front of them now, when we think about our image, prestige, or money instead of helping others, when we blindly follow what others tell us to do instead of observing and drawing conclusions ourselves, when we are not true to who we are, we lose it.
We lose the promise of a life well lived.
- Irrelevant Vaccines and Untested Boosters
Until now, all COVID-19 vaccines and boosters available in America were engineered for the original strain of SARS-CoV-2. Over time, mutations have made this target irrelevant. Now for the first time, boosters and vaccines will have different formulas. But beware. Bivalent vaccines are the latest product of a corrupt system that threatens your health.

On August 31, the FDA authorized new bivalent boosters by Pfizer and Moderna for individuals 12 years and older. At the same time, FDA withdrew the EUA for monovalent mRNA boosters for the same age group. The next day, the CDC signed-off on the distribution of these new booster formulas. There has been no change in Janssen’s monovalent booster authorization, and Novavax does not yet have a booster authorization. The new bivalent boosters are unlicensed, unapproved, and—this part is new—untested in human trials. More about that later.
The new boosters are called “bivalent” because they stimulate immunity against two different targets—the original SARS-CoV-2 strain isolated in January 2020, and the Omicron BA.4/BA.5 strains. “Monovalent” vaccines have not changed; they only stimulate immunity against the original SARS-CoV-2 strain, now largely irrelevant. Monovalent mRNA boosters are no longer available; all mRNA boosters are bivalent. The newly authorized boosters are already listed on vaccines.gov, but unvaccinated individuals cannot get one. You must receive a monovalent primary series vaccine before you can receive a bivalent booster.
The bivalent boosters were brought to market so quickly because they bypassed FDA’s standard process. Manufacturers were not required to present clinical trial data.
We knew this was coming. At its June 28 meeting, the FDA’s Vaccines and Related Biological Products Advisory Committee recommended that new booster formulations be authorized without examination of data by the FDA.
COVID-19 vaccine trials have been flawed. The clinical trials for each of the four authorized vaccines lack long term follow-up. All four vaccinated the control group so that we will never know of vaccine complications that occur more than a few months later. FDA authorized and approved mRNA vaccines without knowing whether the vaccines cause birth defects or whether they are safe to give during pregnancy. The mechanism of major adverse effects such as VITT or myocarditis is still unknown. None of the trials showed that vaccination resulted in a reduction in all-cause mortality. Despite these flaws, FDA has insisted on clinical trials before granting emergency use authorization.
Instead of addressing the flaws and tightening up the process, FDA has decided to do away with clinical trials altogether.
Dr. Paul Offit said he felt the fix was in. “I’ve seen nothing like this,” he said. “Both Moderna and Pfizer presented data during the June 28 meeting, and it was not compelling.” Dr. Offit noted the lack of a control group in the scant data presented. “That’s the obvious thing to do because that’s why you have control groups for your experiment, and I just found it odd that neither presented,” he added. “That bothered me.”
If this bothers Dr. Offit, it should bother you too. Dr. Offit and I have had very different perspectives during the pandemic. In an PBS interview last year, Dr. Offit said that vaccine opponents are the cause of pandemic deaths. Dr. Offit has gone on record in favor of vaccine and mask mandates for school children. As a member of the FDA’s VRBPAC, Dr. Offit has supported most vaccine and booster authorizations, until now. Dr. Offit cast one of the two dissenting votes at the June meeting, and he was so bothered that he co-authored an Op-Ed shortly afterward.
Could these new genetic injections cause unforeseen harm? Of course they can. This blog has warned of the unintended consequences of new technology. There are many examples in medicine of well-intentioned novel therapies having disastrous results, harming many more than they helped. Again, Dr. Offit makes this point, “No one would have predicted myocarditis associated with mRNA vaccines. I don’t think anybody would have predicted this clotting problem so-called thrombosis with thrombocytopenia syndrome. So, humble yourself.”
It will be hard to prove that vaccines cause injury without methodical study. And methodical study is what FDA is eliminating. We may never know the harm caused by these boosters.
There is one thing for sure. With 105 million doses of the new bivalent booster already on order, Pfizer is going to receive a large check from American taxpayers this fall—at least $3.2 billion. Money and corruption are often found together.
Irrelevant vaccines and untested boosters are products of a corrupt system that intends to trap you in an unending cycle of injections, robbing your money before robbing your health.
I saw this in my crystal ball last year.
- Segregation
More than fifty years after the Civil Rights Act of 1964, America still struggles with segregation. Irrational restrictions of freedoms are imposed on unfavored groups by those in power. Is it legal? Yes, unfortunately it is. But it is not right.

First, some factchecks. The idea that vaccinated individuals cannot contract COVID-19 is false. The idea that vaccinated individuals cannot spread COVID-19 is false. We know these ideas are false by the scientific method which compares ideas such as these to real-world observations. We have several notable counterexamples. President Biden, Jill Biden, Anthony Fauci, and Justin Trudeau all recently contracted COVID-19 despite being fully vaccinated and up to date with boosters. Anyone who contracts COVID-19 can spread it to others regardless of vaccination status. To believe that vaccinated individuals cannot contract COVID-19 or spread it to others is to deny science.
Why did vaccines not produce promised protection? There are many reasons. For example, these have always been leaky vaccines. But even more compelling, all vaccines and boosters available today target a virus that no longer exists. COVID-19 vaccine targets were mapped in January 2020. The virus has mutated many times since then. Anyone who received these vaccines are potential transmitters of the current virus. There is no scientific basis for segregation of the unvaccinated.

William L. Moore file photo from 1963. (scanned 02/07/03) Killed in Alabama April 23, 1963 Published April 24, 1963 Evening Sun Walks against Segregation Original Caption On Another March William L Moore was on his way to plea for passage of the public accommodation bill at the General assembly in Annapolis when photo was taken Yet segregation exists. For example, there is a large health care system that prevents some unvaccinated physicians from practicing medicine in its hospitals by terminating their medical staff membership and privileges. It acts summarily, without due process, and without regard to appropriately submitted religious exemption petitions, the same religious exemption petitions which were accepted by other major health systems in the area.

Another example. As part of its back-to-the-office initiative, a major area employer has corralled unvaccinated employees into a single floor, forbidding them to visit to any other floor of their downtown office building.

Although these actions are irrational and unscientific, they are legal. In Biden v. Missouri, 595 U.S. — (2022),the U.S. Supreme Court upheld the CMS vaccine mandate, giving health care systems broad authority to adjudicate religious or health exemptions for workers who do not wish to be vaccinated. Similarly, employers have broad legal authority to impose restrictions on employees, even irrational ones, so long as those restrictions are not based on a federally protected status such as race, color, religion, sex, or national origin. We have been here before.
In Plessy v. Ferguson, 163 U.S. 537 (1896), the U.S. Supreme Court affirmed the practice of segregation by race so long as separate accommodations were equal, which, of course, they never were. Prior to the Civil Rights Act of 1964, employers had broad legal authority to impose restrictions on employees, even irrational ones, even restrictions based on race, color, religion, sex, or national origin.
Now, as then, misinformation fuels these irrational policies. Now, as then, the same irrational arguments are heard: “Those people are unclean”; “They spread disease”; “It’s in their genes.”
Now, as then, legal does not make right. Unscientific segregation, coerced consent, and irrational discrimination are unethical. These are the methods of bullies and lynch mobs, not freedom loving patriots.
If you have been the victim of segregation, please share your story in the comments below. The readers of this blog want to hear from you.
- Institutionalized Misconceptions

The CDC quietly changed its COVID guidance last week. In an August 11 update to Isolation and Precautions for People with COVID-19, the CDC removed the vaccination advantage for ending COVID-19 isolation. Now the CDC expects everyone to follow the same isolation guidance, regardless of vaccination status. Yet even its newest guidance perpetuates myths that extend the COVID emergency unnecessarily.
Here is the new guidance. If you suspect you have COVID-19, you should test. Isolate until you receive your test result. If your test is negative, end isolation. Asymptomatic individuals with a positive test should isolate for five days and wear a mask for ten. If your test is positive and you have symptoms, isolate for five days from the first day of your symptoms or for 24 hours after you are fever-free, whichever is longer. Mask for ten days. Better yet, mask until you have had two negative antigen tests 48 hours apart.
Previously, CDC recommended different isolation protocols depending on vaccination and booster status. Now there is no difference, another tacit admission that the vaccinated and unvaccinated spread infection similarly. This is a softening of its once bellicose “Pandemic of the Unvaccinated” position, and not the first time either. In the last paragraph of a June MMWR report, the CDC admitted, “Despite the introduction of highly effective vaccines and medications to treat COVID-19, by the end of the study period, COVID-19 continued to cause substantial morbidity and mortality.” Hopefully, this new direction will reduce fuel for those actively practicing health discrimination against the unvaccinated, or against the vaccinated but not up-to-date.
I am not holding my breath. There continues to be a lot of momentum in that direction.
Despite this small positive, the new guidance continues to perpetuate misconceptions that have been institutionalized within the CDC. Here are three examples.
There is a test for COVID-19. The CDC confuses a SARS-CoV-2 test with COVID-19, something this blog has warned against since the early days of the pandemic, but which has become an institutionalized misconception at the CDC. There is not a test for COVID-19. Symptoms are necessary for diagnosis.
Asymptomatic individuals should be tested. Different guidance for those with and without symptoms implies a recommendation for testing asymptomatic individuals. “Asymptomatic spread” is an unsubstantiated idea at best and deliberate fearmongering at worst. Guidelines that promote asymptomatic testing perpetuate the myth that “asymptomatic spread” is a real concern, effectively prolonging the emergency. Testing should be limited and focused.
Tests can determine when to end isolation. The updated guidance uses test results instead of symptoms to end of the isolation period. This misconception relies on the assumption that an individual who has tested negative is unlikely to spread infection. The fallacy of this assumption is embedded in the guidance, which requires two consecutive negative antigen tests to end masking. Why two tests? Antigen tests have low sensitivity, meaning lots of false negative results. If the first test is not reliable, should the second test be any better? “Past performance is no guarantee of future results.”—that works for investing and for testing. The guidance might as well say, “Flip a coin every 48 hours; leave your mask on until you get two heads in a row.” SARS-CoV-2 tests do not test for cure of COVID-19.
Many people just ignore the CDC, but there are those who live in trauma and fear unnecessarily. Misconceptions institutionalized by the CDC trap those individuals in a cycle of stress and panic. It is time for sensible, uncomplicated, time-tested guidance.
If you feel sick, stay home. When you feel better, get on with your life.
Stop scaring people already.
- Am I Up to Date?

Government health policy says Americans should be “up to date” with COVID-19 vaccines, but what does that mean? To answer this question, I had a conversation with CDC’s website. CDC responses are copied verbatim, correcting only misspellings and grammar for ease of reading. Use the links if you want to check the responses for context.
KH: Why should I get a COVID-19 vaccine?
CDC: COVID-19 vaccines available in the United States are effective at protecting people from getting seriously ill, being hospitalized, and even dying.
KH: Then all I need is a vaccination, right?
CDC: COVID-19 vaccines available in the United States are effective at protecting people—especially those that are boosted—from getting seriously ill, being hospitalized, and even dying.
KH: You’re saying that vaccination isn’t enough—I need a booster too?
CDC: You are protected best from COVID-19 when you stay up to date with the recommended vaccines. You are up to date with your COVID-19 vaccines when you have received all doses in the primary series and all boosters recommended for you when you are eligible.
KH: How do I know what boosters are recommended for me?
CDC: Vaccine recommendations are different depending on your age, the vaccine you first received, and time since last dose.
KH: Let’s say I got Pfizer. When am I fully vaccinated?
CDC: Two weeks after final dose in primary series.
KH: How long do I have to wait after my first dose before I can get my second one?
CDC: Three weeks (or 21 days) after the first dose.
KH: First dose, wait three weeks, then second dose, then wait two weeks, then I’ll be fully vaccinated, right?
CDC: People ages 6 months through 64 years, and especially males ages 12 through 39 years, may consider getting the second primary dose of an mRNA COVID-19 vaccine (Pfizer-BioNTech or Moderna) eight weeks after the first dose.
KH: Why is that?
CDC: A longer time between the first and second primary doses may increase how much protection the vaccines offer, and further minimize the rare risk of heart problems, including myocarditis and pericarditis.
KH: Myocarditis! That sounds serious.
CDC: There is a rare risk of myocarditis and pericarditis associated with mRNA COVID-19 vaccination, mostly among males ages 12 through 39 years. Those who have been diagnosed with myocarditis should consult with their cardiologist (heart doctor) about return to exercise or sports.
KH: I don’t want to stop playing sports, so maybe I should wait eight weeks before my second shot. Do I need a booster?
CDC: One booster, preferably of either Pfizer-BioNTech or Moderna COVID-19 vaccine, at least five months after the final dose in the primary series.
KH: I’m 59–just one booster?
CDC: Second booster of either Pfizer-BioNTech or Moderna COVID-19 vaccine for adults ages 50 years and older, at least four months after the first booster.
KH: Primary series—two shots—then two boosters. I need four shots to be up to date? What if I’m immunocompromised?
CDC: First dose-primary series; second dose-primary series three weeks after first dose; third dose-primary series at least four weeks after second dose; forth dose-booster at least three months after third dose; fifth dose-booster at least four months after forth dose.
KH: Five doses! Is that safe?
CDC: The safety, effectiveness, and benefit of the third primary dose in people who are moderately or severely immunocompromised continues to be evaluated.
KH: Let me review. You’re saying that to be up to date and fully vaccinated in the safest possible way, I should get my first shot, wait eight weeks (or did you say three weeks?), get my second shot, wait four more weeks (or is it eight weeks?), get my third shot (I’m immunocompromised, remember?), then wait three months (or is that five months?), get my fourth shot, wait four more months, then get my fifth shot. How can I afford so many shots?
CDC: COVID-19 vaccines are available for everyone ages 6 months and older at no cost.
KH: Great! Vaccine makers are sacrificing profits to give away vaccines to Americans. How patriotic!
CDC: Vaccines were paid for with taxpayer dollars.
KH: Oh, I see. COVID-19 vaccines are not free. Taxpayers are paying vaccine makers for the shots given to fellow citizens…
CDC: …to all people living in the United States, regardless of health insurance or immigration status.
KH: You mean my tax dollars are paying for vaccines for all those people crossing the southern border illegally?
CDC: Jurisdictions (state, tribal, local, and territorial) cannot add U.S. citizenship requirements or require U.S. citizenship verification as a requirement for vaccination.
KH: Let me get this straight. The government takes money from me and gives it to vaccine makers so that anyone living in the United States can access vaccines. What do you call that?
CDC: If anyone asks you to pay for access to a COVID-19 vaccine, it’s a scam.
KH: You said it.
- Too Much Testing

Frustrated by misconceptions about SARS-CoV-2 testing, I began my career as an amateur blogger nearly two years ago. I am motived by similar frustrations to write this blog today, but the source of today’s frustration is someone who should know better—the doctor to the President of the United States.
Joe Biden announced on Thursday, July 21, that he tested positive for COVID-19, despite being double vaccinated and double boosted. Setting aside this fact as evidence that vaccination does not prevent future infection, that vaccination cannot eradicate the virus, and that current vaccinations stimulate immunity against the wrong target, I want to focus on the misuse of testing to perpetuate the COVID emergency.
On Wednesday the President’s doctor, Kevin O’Connor, DO, FAAFP, announced that Mr. Biden had repeatedly tested negative for SARS-CoV-2, and he lifted strict isolation measures. But on Saturday, the doctor reported a positive antigen test. He declared the President in relapse, blaming the same “Paxlovid rebound” that plagued Dr. Anthony Fauci during his infection in June. In case you are wondering, Dr. Fauci also reports being fully vaccinated and up to date on boosters, and according to Dr. Fauci, his second round of symptoms were worse than his first. In case you are also wondering, I had a single Janssen vaccine without booster ten months before my infection, and I suffered no “Hydroxychloroquine rebound” when I had omicron. And I did not test.
Let me say this as plainly as possible.
SARS-CoV-2 tests are not tests of cure. They can tell you when someone is first infected by the virus, and that is all. They cannot tell you when someone is rid of disease and no longer infectious. The diagnosis of COVID-19 requires evidence of respiratory disease and a positive test for SARS-CoV-2. Either one without the other is not COVID-19. Despite the CDC’s redefinition midway through the pandemic, there is no laboratory test for COVID-19.
There are two types of SARS-CoV-2 tests—PCR tests and antigen tests. PCR tests are highly sensitive, but positivity can persist for up to three months after infection. During this period, tests are not reliable to identify reinfection, since any positive might just be remnants of the old infection. Antigen tests are much less reliable. Although an initial positive antigen test may indicate infection, negative tests do not mean a person is free of infection. This has not changed since EUA testing began in 2020.
If the President is subjected to daily testing, he may be diagnosed with many relapses in coming weeks, but that does not mean he still has COVID-19. For that, doctors must rely on clinical observations. The President’s doctor should know this. He must know this.
Testing is being misused to perpetuate the COVID-19 emergency in our nation. This episode illustrates the dangers of testing misuse and overuse. We need a return of common sense, as much among doctors as among the public. Testing should be limited and focused.
We all know when we feel sick. If you do, stay home, and seek early treatment, because early treatment keeps you out of the hospital. I used the Zelenko protocol when I had Omicron.
When you feel better, return to your life. We do not need tests for that.
- The Art of Science
“When all was finished, it cannot be denied that this work has carried off the palm from all other statues, modern or ancient, Greek or Latin; no other artwork is equal to it in any respect, with such just proportion, beauty and excellence did Michelagnolo finish it.”
Giorgio Vasari, 1550
Michelangelo’s David, 1501-1504 David, the breathtaking masterpiece by Michelangelo, represents the pinnacle of Renaissance sculpture, the result of countless hours in practice, planning, and observation of human forms. Carved from a single massive block of Carrara marble which had been discarded by other sculptors, Michelangelo’s creation embodies confidence and power. The body’s position, the facial expression, and even the veins popping in the neck all betray a determined youth on his quest to slay a giant. You can learn a lot of anatomy, physiology, and psychology by studying David. But nobody would confuse the statue with a living man.
And why not?
This statue never moves, it is twice the size of a man, and it feels like cold stone instead of flesh. Its proportions are wrong, perhaps intentionally so. Cut it open, and you will find dust instead of a beating heart. Michelangelo’s David is not a man. It is just a model that provides ways to think about man.
Science is like that. Like art, science is a creative endeavor. Scientists do not discover truth any more than Michelangelo discovered David inside the stone.
For example, Sir Isaac Newton did not discover the law of gravity; he invented it. His model replaced Aristotle’s 2,000-year-old idea that things fall because they seek their natural place in the universe. Newton proposed that bodies attract each other in proportion to the product of their masses and inversely to the square of the distance between them [Fg = G(m1m2)/r2]. Both ideas explain why a cannonball dropped from a tower goes down, but only Newton’s model explains why the moon hangs in perpetual freefall around the earth.
Newton’s invention is elegant and useful, even taking men into space, but it is not true. For example, Newton’s model fails to explain the wobbly orbit of Mercury. To correct the deficiencies of Newton’s theory, Albert Einstein invented a model of gravity in which objects bend the unified field of spacetime, pushing them towards each other. Although Einstein’s Theory of Relativity explains the paradoxical orbit of Mercury, even his invention has shortcomings. In the subatomic world of Fermions and Bosons, Einstein’s theory just doesn’t work.
A model does not have to be universally true to be useful. Despite its many limitations, science does two things incredibly well. First, it shapes what you believe by informing on what is not true. This is because the scientific method is an iterative process that tests ideas against independent observations. Second, brilliant scientists compile observations into theories of various aspects of the universe. In this way, scientists and artists have much in common. Both create models that provide ways to conceptualize the complex, stimulating new thoughts and ideas.
Scientific models should not be confused with truth. Truth is all around you, in nature. Scientific models are ways to think about nature when you close your eyes, when your viewpoint is obstructed, when you cannot see nature clearly. Scientific models are merely shadows like the ones on Plato’s cave. The Allegory of the Cave described the art of science long before scientific principles were articulated.
- Against the Rules
FDA made significant changes to COVID-19 vaccines available in the United States last week. In its recent actions, the FDA displays pattern of blatant rule breaking that indicates negligence and corruption. Here are three examples.

Pfizer. FDA gave license to vaccinate middle-schoolers twelve years and older with COMIRNATY by its supplement approval letter of July 8, 2022. This approval was issued in response to Pfizer’s submission of pediatric Study C4591001 regarding safety and effectiveness of COMIRNATY in children 12 through 15 years of age. However, Pfizer reports that this study relied on data from a trial using 16 to 25 year-olds conducted prior to Delta and Omicron surges, raising questions regarding its relevance.
FDA rules require manufacturers to inform FDA within 6 months of “a permanent discontinuance in manufacturing”, or “an interruption that could lead to a meaningful disruption in the supply of the product in the United States” (page 7, lines 208-210), even if the manufacturer decides to cease production for business reasons (lines 221-222). COMIRNATY has never been available in the United States in the eleven months since initial approval. I am not an attorney, but this seems like a meaningful supply disruption of the licensed product to me, which should trigger a reconsideration of the vaccine’s license. An expansion of COMIRNATY’s license while the product is still unavailable violates the spirit, if not the letter, of FDA’s own rules. Instead, the approval appears to be merely a merit badge providing a marketing advantage to Pfizer without changing that fact that no approved vaccines are yet available to Americans.

Novavax. The predicted authorization of the all-protein Novavax vaccine happened with fanfare last week. FDA’s press release welcomed the arrival of “another option” for Americans, and assured that “the American public can trust that this vaccine, like all vaccines that are used in the United States, has undergone the FDA’s rigorous and comprehensive scientific and regulatory review.” I have issues with both statements.
The use of emergency use authorization to provide “another option” violates the rules governing emergency use authorizations. The purpose of the EUA is to make products available when “there are no adequate, approved, and available alternatives.” There are approved alternatives—COMIRNATY and SPIKEVAX—which are, by manufacturers’ choice, unavailable. But adequate alternatives are available. Search vaccine.gov to see whether you can find vaccines in your area. If you cannot, please let me know. If you can, another unapproved option is unneeded.
The assurance of “rigorous and comprehensive scientific and regulatory review” is misleading, since that describes the approval process, not the authorization process. EUA is for emergencies, like bailing water out of a sinking ship. “Rigorous and comprehensive” describes a process to assure seaworthiness before putting the ship into water and results in a license to sail. Novavax has no license. It has not been through a truly rigorous and comprehensive scientific and regulatory review.

Moderna. Authorization letters require manufacturers to comply with section 502(a) and (f) of the FD&C Act, which prohibits false or misleading labelling. Yet children ages 6 through 11 are to be vaccinated with Moderna Purple, which is labelled “BOOSTER DOSES ONLY” because Moderna Teal is still unavailable. Unreliable labelling is a setup for medical error, which is why the rules prohibiting misleading labels are so clear. Instead of insisting that Moderna relabel product before distribution, FDA issued a “Dear Healthcare Provider” letter, instructing caregivers to ignore the printed label.

Vaccine chart, updated July 16, 2022. This is the current state of vaccines in America. We did not get here honestly. Instead, we got here by bending, twisting, and breaking the rules established to keep us safe.
FDA is a law enforcement agency that should respect rules. If you come under FDA’s jurisdiction, you rigorously follow its rules and regulations because FDA has the power to shut you down. Just ask Abbott Nutrition, the operator of the Michigan baby food plant forced to cease production earlier this year. The resulting baby formula shortage is a serious emergency, yet there have been no emergency use authorizations for manufacturers racing to have new product approved. Meanwhile, we still have an emergency declaration that short-circuits the process for vaccines.
The FDA has compromised its rules related to vaccines. It is a clear signal of negligence and corruption. There is something pathologic at the FDA.
- Medical Publications Bow to a Political Narrative Causing Loss of Public Trust
Publications in top-tier medical journals must comply with a narrative. As a prerequisite for publication, authors must affirm that universal vaccination is the best response to pandemic, and that the benefits of vaccination outweigh any harm it causes. Even articles that describe vaccine injuries must minimize their risks in deference to the goal of universal vaccination. This misuse of the medical literature suborns the mission of journals to a political agenda, squandering the trust they once enjoyed.
I noticed this trend during research for these blogs. Here are a few examples to give a flavor of the narrative.
- In a recent review of clotting complications caused by vaccine published in Journal of Stroke and Cerebrovascular Diseases, Kakovan et al. end their article by saying, “Finally, since the advantages of COVID-19 vaccination outweigh the risk of stroke or any other neurological complication, the public should be reassured that the vaccination program is still the best way to combat COVID-19.” The article gives no support for this conclusion. It is as if the authors knew that homage to this dogma was the price of publication.
- In a Reviews in Medical Virology article presenting data showing that vaccination causes a 13.6 times increase in myocarditis among 16-19 year-old males, Faziollahi et al. conclude that these complications are “rare,” missing this obvious data signal.
- “VITT [Vaccine-Induced Immune Thrombotic Thrombocytopenia—the blood clots caused by vaccine] appears to be a very rare side-effect of vaccination…” Perry, et al. in The Lancet.
- “The very low prevalence of this complication of vaccination, however severe, relative to the benefits of preventing Covid-19 (a condition with 1 to 2% mortality and potential long-term sequelae) must be emphasized.” Clines and Bussel in New England Journal of Medicine.
- “Independent safety reviews by regulatory authorities of available clinical and real-world evidence have concluded that the benefits of AZD1222 outweigh the potential risks.” Falsey et al. in New England Journal of Medicine.
- “The thromboembolic complications do not represent a contraindication to complete the vaccination cycle…” and “The vaccination for SARS-Cov-2 is essential to overcome the pandemic…” Serrao et al. in Journal of Thrombosis and Thrombolysis.
The narrative is fully stated in this quote from an article published in Journal of Clinical Medicine to help practitioners provide “evidence-based counseling to their often-alarmed patients” who have new blood clots after vaccination. Abrignani et al. conclude,
“All scientific societies emphasize the value of continuing vaccination programs to protect patients from severe forms of COVID-19 and to slow the circulation of the virus and its variants. Vaccine hesitancy risks regressing progress in infectious disease control. Abstention is not an option, as it results in a failure to assist a large population that remains in danger. Action, with increased vigilance, is the best solution in our public health mission.”
Medical journals should be places of conflict, where ideas clash, paradigms are upended, and the status quo is challenged. The New England Journal of Medicine claims, “Our mission is to publish the best research and information at the intersection of biomedical science and clinical practice and to present this information in understandable, clinically useful formats that inform health care practice and improve patient outcomes.” But the crossroads of biomedical science and clinical practice is not a static location, unchanging over time. Without medical journals exposing dangers of established practice, physicians might never have learned that diethylstilbestrol treatment causes cancer or that thalidomide therapy causes birth defects.
Today’s medical journals have devolved into a repository of orthodoxy where platitudes are exchanged among the sanctified. They bow to a narrative that coincides with a political agenda, mocking the missions of these publications. The trust accumulated from two centuries of diligence and integrity has been lost in a few months.
The erosion of trust does not stop with the journals. It extends to my entire profession of physicians. Yet too few of my colleagues have acknowledged this trend. Instead, most parrot the narrative to their patients. Why? Are they afraid they will never be published again? Are they afraid they will be ostracized from the society of physicians and scientists? Or are they just too lazy to observe and think for themselves?
Physicians have a sacred duty to the patient in front of them. This duty requires honest observation, independent thought, and attention to the patient’s best interest. Without these, we deserve the loss of public trust.
- I Had Omicron
I am pretty sure I had Omicron in January. I say “pretty sure” because I did not confirm infection with a PCR test. By now you know why I think most of these tests are unnecessary. It felt like a cold, and a rather mild cold at that. Most people in my family had the same symptoms; I encouraged them not to test, and they did not. I remember that people around me felt sick too—some took time off work, some blamed allergies. I am pretty sure it was COVID.
We were on vacation at the time, lest you worry I spread my infection to sick people, although I did take a flight home while still stuffy. Masks on airplanes were still mandatory at the time.
But I hedged my bets. I took hydroxychloroquine for a week. I tripled my daily vitamin D, did daily nasal washes, and started taking Dr. Zelenko’s Z-stack vitamins (I haven’t stopped taking those). I never lost taste; I never lost smell. It took me a month to shake the sniffles, but nothing else lasted more than 36 hours.
My wife, Liz, never felt ill. She has lupus and has taken hydroxychloroquine for years. Maybe that is why.
Back up a bit. I am pretty sure we avoided COVID before then. Liz and I were extra careful. She has an autoimmune disease, and I work near sick people. We weren’t taking any chances. We cancelled vacation plans (not the vacations, just the plans), and found we could live quite comfortably—enjoyably, even—at home. Alone. We did not go out to eat. We stopped shopping in the mall. We became friends with Doordashers, the Amazon Delivery persons, and other deliverers of our on-line shopping selections—at an appropriate social distance, of course. We picked up groceries curbside. We went out rarely, and when we did, we masked religiously.
We both took Johnson and Johnson vaccines in March 2021, and my wife instantly had a lupus flare. The migraines which she had previously experienced once a month became daily, painful affairs. She had to change medications to a more powerful and (any surprise?) much more expensive drug. She still has ringing in her ears and extra pain in her joints that she dates from the shot. Migraines are no longer daily, but still more frequent than before. I was skeptical of mRNA technology from the start, but I regret the decision to take a vaccine.
I am a curious person, and life had presented us with the opportunity to study something that had never been studied before. I began measuring antibody levels in friends and colleagues who had made a variety of choices about vaccination and COVID precautions. We identified some people who had had COVID but did not know it. We identified people who had COVID after vaccine. We learned early on that Moderna produces the highest immune response, and we learned that vaccine did not add much immunity to people who had disease. Some people, including me, had little immune response to vaccine.
The antibody tests available then were not very good, and they kept changing, making it impossible to track serology over time. That is why Liz and I joined the TXCares study. After answering some questions, we measured the S-protein and N-protein antibodies in our blood three times over six months. Here are our results:

S-antibodies (S-Ab) can come from either infection or vaccine, but N-antibodies (N-Ab) can come only from infection. Since our S- and N-antibodies increased in February, I am pretty sure we had COVID in January during the Omicron wave.
Antibody tests are still not very good. For example, I consider the change in N-protein levels from nil to barely detectable significant, even though our levels did not reach the arbitrary positive level of 1. But at least these tests were consistent over time, and the results corresponded with our clinical history.
How do I feel now? For starters, we are not scared of COVID anymore. We do not mask (except at the hospital), we do not avoid people, and we shake hands again. The only current lifestyle impact is the continued coercion to vaccinate. If an activity requires a vaccine card, we avoid it. That means we still do not travel internationally, and we do not patronize certain entertainment venues, including, regrettably, venues we once loved. But that is it. Otherwise, we are normal again. Well, maybe not quite. My wife’s lupus is worse, and I have a positive d-Dimer, but that is a story for another day.
Antibody levels consistently and reliably inform on immunity, yet they are spectacularly underutilized. Perhaps this is because they are spectacularly inexpensive. Consistent, reliable, and actionable information is not what the game is about right now. If spike protein antibodies are a good thing, and I am still not sure they are, Liz and I have plenty to spare. But we were going to have them sooner or later. COVID is not going away until most of us catch the virus. Vaccinated or not, most of us have.
- Regulatory Capture
Up to now, all the vaccines have been the same. The only differences in the vials are the concentrations of genetic material for various age groups and boosters. As the virus continues to mutate at a rapid pace, current vaccines are becoming irrelevant. That may be about to change, but not for better. The roadmap to release of future vaccine versions will be the subject of the FDA’s Vaccines and Related Biological Products Advisory Committee meeting on Tuesday. This plan could open the door to genetic engineering without safety oversight.

Simplicity and standardization reduce error, yet vaccine rules are becoming more complex. Instead of mandating standardization, the FDA has allowed manufacturers to establish packaging, dosing, and interval parameters. This is the result of regulatory capture—regulators overtaken by those they are charged with regulating. Regulatory capture has caused FDA to authorize so many versions that it is easy to forget there are still just three vaccines available in the United States.
Pfizer, Moderna, and Janssen vaccines have not changed since their introductions. All three are designed to produce immunity against a virus which is no longer a threat. Although the many different vials in the Pfizer and Moderna vaccine families make it appear these companies have been hard at work making new vaccines, they only adjusted the product concentrations and doses for different age groups and boosters without the slightest change in the immunity target. We’re skating to where to puck has been, not to where it is going.
The FDA and vaccine manufacturers are aware of the problem. Like the needlessly complicated vaccine landscape, their solution will be another example of regulatory capture. If approved, future Covid-19 vaccines versions will skip clinical trials. The manufacturer can change the genetic material in these vaccines without understanding the consequences of the change. If you want plan details, read this Substack article by Dr. Toby Rogers of Brownstone Institute.
Why is this dangerous? Afterall, if we are going to keep up with this virus, shouldn’t we give scientists the freedom to engineer the vaccines on the fly?
The first problem with this idea is that scientists do not know what they are doing. Because the understanding of genetics and immunology is incomplete, we cannot expect scientists to flawlessly produce genetic code that is safe for human injection. If I download and install a hack I find online, the worst outcome is a bricked phone (it’s happened; ask my wife). If genetic engineers make a mistake, the consequences are frightful—think Zombie movies, Frankenstein, and Jurassic Park. Afterall, they are tinkering with the operating system of life. Genetic engineering should require more oversight, not less.
The motives of vaccine manufacturers represent a worse problem. These companies have a duty to their boards and shareholders that supersedes the health and wellbeing of their customers. We regulate the healthcare industry for this reason. If we give pharmaceutical companies license to sell untested versions of genetic code, they will use it to bulk up balance sheets. Honest clinical trials are the only way to check these corrupt intentions.
We must get integrity back into the oversight and approval process, and we do this by getting the money and corruption out. Safety cannot be ensured when studies performed at universities and published in journals by scientists are presented to advisory committees. At least not when the company pays for the study, endows the university, advertises in the journal, pays royalties to the scientists, and funds committee member projects. These cozy arrangements must end. Anti-kickback laws must apply to all parties in the biomedical-industrial-regulatory complex.
- Why Is the Vaccine Landscape So Complicated?
Ten months ago, I posted the first Quick Chart on COVID Vaccines to aid in understanding the increasingly complex vaccine landscape. Today, I’m revising the chart for the sixth time to include new information contained in fourteen Fact Sheets released by the FDA on Friday. These Fact Sheets cover eleven vaccine versions from three manufacturers, each with unique cap color, label border color, dilution volume, dose volume, and dose interval, all dependent on the age of the recipient. The Fact Sheets supersede (see under “Storage and Handling, page 3) package inserts and vial labels which are now obsolete and unreliable. These emergency vaccine authorizations cover all Americans, literally cradle to grave, from age 6 months until death. The exploding complexity is based on whim, not science, as Dr. Anthony Fauci acknowledged last week.

Vaccine Chart compiled from Fact Sheets for Health Care Providers, June 2022 The chart above is compiled from all Fact Sheets for Health Care Providers, which you can find in these indexes for Pfizer, Moderna, and Janssen. I have done diligence to ensure accuracy, but given the extreme complexity, I cannot be liable for errors. Errors on the chart could be embarrassing to me. Errors in administration of vaccine could have disastrous consequences for vaccine recipients, so the FDA also published wall charts for Pfizer and Moderna vaccine families for reference.

Pfizer Wall Chart 
Moderna Wall Chart While tabulating information, I noticed some interesting language.
First, FDA gives a new justification for the persistence of Emergency Use Authorizations for vaccines that have approved versions. Footnote 16 of the reissued ModernaTX Authorization Letter reads, “Although SPIKEVAX (COVID-19 Vaccine, mRNA) and Comirnaty (COVID-19 Vaccine, mRNA) are approved to prevent COVID-19 in certain individuals within the scope of the Moderna COVID-19 Vaccine authorization, there is not sufficient approved vaccine available for distribution to this population in its entirety at the time of reissuance of this EUA.” Of course, this is a sham. Moderna will never produce enough SPIKEVAX for distribution to the entire population so long as it can produce vaccines for emergency use which have liability protection.
Second, Moderna Teal, packaged for age 6 through 11 years, is not currently available (see Fact Sheet bullet at top of page 2). Instead, 6 through 11-year-old children are to receive Moderna Purple, labeled “BOOSTER DOSES ONLY,” as their primary series vaccine (see Fact Sheet bullet at bottom of page 1). Presumably, the Moderna Purple and Teal formulations are the same, but “Moderna COVID-19 Vaccine is not authorized to provide booster doses to individuals 6 years through 11 years of age.” Only Pfizer Orange is authorized for booster doses in children under 12 years old.
Finally, all other mRNA vaccines have a two shot primary series with a third shot for the severely immunocompromised, but not Pfizer Maroon. All infants and toddlers get a three shot primary series when vaccinated with Pfizer.
Why is this so complicated? There must be very sophisticated data and detailed scientific analysis to produce these dosing rules for primary series and boosters. Some really smart people must have worked all that out for us.
No. These rules are based on conjecture and assumption, not science. For example, according to Dr. Fauci, there are no studies supporting boosters for kids, yet boosters for kids were authorized by FDA last week. But don’t take my word for it. Watch for yourself and decide.
If science is not driving the complicated vaccine landscape, there must be another reason. My hunch—follow the money.
- Why Vaccinating Kids Is an Emergency
This week the FDA’s Vaccines and Related Biological Products Advisory Committee will meet twice to consider COVID-19 emergency use authorizations for children. On Tuesday, June 14 the committee will consider Moderna’s request to vaccinate children aged 6 through 17, and on Wednesday, June 15, the committee will consider requests from Pfizer and Moderna to vaccinate all children and infants down to six months of age. Infants and children have the lowest death rate from COVID and the highest risk for adverse health consequences, so why is vaccinating children an emergency?

Kids die from COVID-19, but the death rate is astonishingly low, especially when compared to other childhood risks. According to the American Academy of Pediatrics, between 0.00% and 0.02% of all COVID-19 cases in U.S. children result in death. As of June 2, 2022, there have been 1,049 childhood deaths from COVID-19, total. By comparison, in 2019 nearly 2,400 teenagers died in car accidents, and 1,250 infants died of SIDS. Yet, any childhood death is tragic. If vaccination reduces death from COVID-19, why not vaccinate our children to reduce even this tiny risk?
An honest risk-benefit analysis requires examination of both sides of the equation, so we must first look at the risks of vaccine in children.
Many of these risks are still unknown. The kids who have been vaccinated have not grown up, entered the workforce, or had children. Nevertheless, sobering data is emerging. Vaccinated males between 16 and 19 years old have a 13.6 increase incidence of myocarditis compared to historical norms. So far, there have been 52 deaths reported to VAERS after COVID-19 vaccine in children aged 6 months to 17 years. Reports of blood clots in vaccinated children are beginning to surface, unsurprising since thrombotic vaccine risks in adults are well established. According to data released by Pfizer, vaccination is associated with increased miscarriages. Perhaps most compelling, the study funded by Pfizer and published in the New England Journal of Medicine to support vaccine administration in children shows no improvement in all-cause mortality (see table S2).
And we still have those risks of the unknown. Read again how a seemingly harmless hormone caused cancer in the daughters of women injected with it.
If it is hard to reconcile the risk-benefit in favor of vaccinating kids, there must be another reason for the push to do so. Perhaps it is not a health emergency for children but a liability emergency for vaccine manufacturers. Vaccine liability protection will evaporate once the COVID-19 emergency is lifted, but childhood vaccines enjoy special liability protection.
Emergency Use Authorization makes unapproved products—vaccines, tests, treatments, and so on—available during a public health emergency when there is nothing approved that works. Manufacturers do not want to be liable for unintended consequences of unapproved products. Although an EUA does not by itself provide product liability protection, there is a loophole. The Secretary of HHS can issue a PREP Act Declaration which absolves manufactures from all liability except willful misconduct for claims “resulting from administration or use of countermeasures to diseases, threats and conditions.”
The HHS Secretary issued a PREP Act Declaration for COVID-19 that includes vaccines, granting liability protection for as long as the emergency lasts. It has been extended 10 times. But the emergency cannot go on forever. The end game is permanent liability protection.
In 1986, congress passed the National Childhood Vaccine Injury Act (NCVIA) which created the National Vaccine Injury Compensation Program, “a no-fault alternative to the traditional legal system for resolving vaccine injury petitions.” If you can prove vaccine injury, you can ask for financial compensation from the fund rather than file lawsuit against the manufacturer. This system is open to “any individual, of any age, who received a covered vaccine,” but there is a catch:
For a vaccine to be covered, the Centers for Disease Control and Prevention (CDC) must recommend the category of vaccine for routine administration to children or pregnant women…
Heath Services and Resources Administration definition of Covered Vaccines.Currently, COVID-19 vaccine manufacturers have liability protection because they are selling unlicensed products under emergency use authorization. But once these products are recommended for routine administration to children or pregnant women, then vaccine liability protection will continue under the NCVIA, even when the emergency declaration is lifted.
Now we know why vaccinating children is an emergency. At the same time, we have stumbled on the answer to a question I asked a few weeks ago. Why does CDC recommend COVID-19 vaccines to pregnant women, despite the explicit Fact Sheet statements (see page 44) warning of the lack of safety data?
The answer to both questions is the same. Like vaccinating pregnant women, vaccinating children gives manufacturers a pathway to permanent liability protection.
- The Novafix
On Tuesday, June 7, the Vaccines and Related Biological Products Advisory Committee (VRBPAC) will consider evidence supporting emergency use of Novavax COVID-19 Vaccine. The outcome of these proceedings is nearly certain. The committee’s endorsement will be followed by a swift EUA letter from the FDA and recommendation by the CDC. The only uncertainty is how many times committee members will contradict previous statements in their sycophantic rush to fawn over this new all-protein vaccine.

FDA Placeholder for Novavax Fact Sheet, June 5, 2022. FDA webmasters have already been hard at work, excavating a location for the new vaccine’s authorization documents. Click here today and you will see the placeholder for the Novavax Recipient-Caregiver Fact Sheet. Next week, the same link will bring up the actual documents.
Wall Street is also lining up behind the new vaccine. According to a recent article published on Nasdaq.com, “So far, in all previous global regulatory approvals in other regions, there has been ‘minimal to no debate’ on the highly effective and safe credentials of the vaccine as shown in the 3 large-scale Phase 3 studies. And going by previous examples of such EUA FDA panels, following a positive vote by VRBPAC panelists, Mamtani [an analyst working for B. Riley Financial] expects a ‘prompt FDA approval.’”
The article continues, “Accordingly, Mamtani reiterated a Buy rating on NVAX shares, backed by a $181 price target. Investors stand to take home about 227% gain, should the target be met over the next 12 months.” This is Mr. Mamtani’s recommendation, not mine. I am a practicing pathologist and do not give financial advice. I only reference this article to restate a previous point—this is about the money.
The fix is in. As Wall Street proclaims this new vaccine “highly effective and safe,” expect committee members to opine at length that the new vaccine is new technology. Since it does not use mRNA, it should be readily accepted by the unvaccinated holdouts by removing their objection to gene therapy. Obsequious committee members will heap praise on the company for producing this missing piece to the pandemic puzzle.
Their praise will create a contradiction that undermines the committee’s credibility. If the war on pandemic requires another vaccine, then the vaccines currently available must not be the panacea we were told previously. To believe what the committee will say this week, we must stop believing that what the committee said previously about mRNA vaccines being “safe and effective.” Maybe they are not safe enough or not effective enough. Otherwise, why would a new vaccine meet requirements for emergency use authorization? And if we must stop believing something they have said before, why should we believe them now? This is not science. This is politics.
Tuesday’s committee discussion will not recognize any of the problems with the Phase 3 trial published in the New England Journal of Medicine earlier this year. They will not consider the failure of vaccine to reduce all-cause mortality, the high number of short-term adverse effects, or the elimination of the control group after two months. They will simply parrot the study’s conclusion of “safe and effective” without critical examination of the study’s flaws, and without mentioning that the study that was funded by the vaccine maker.
By the end of the week, a new vaccine will be available to Americans. The new vaccine will not met rigorous approval standards, but it will have the same manufacturer liability exemptions as the other EUA vaccines. Novavax stands to make a lot of money with minimal risk. However, there is little evidence that this new vaccine will create a health benefit for Americans.
- Because I Say So
The fascists tell us what to think. They expect us to follow arbitrary commands based on the strength of their word alone.
Case in point. NPR recently published an article supporting the “Pandemic of the Unvaccinated” narrative. The article claims there were nearly 319,000 excess deaths caused by the failure to universally vaccinate all adult Americans. Why should we believe this? “Because I say so.”
This chart from the article summarizes the report:

The lines charting actual and estimated deaths diverge in August 2021. Actual deaths have steep slopes in October 2021 and January 2022, corresponding to the waves of delta and omicron variants. The modeled deaths for the universal vaccination scenario show barely a bump during these times, implying that vaccination would have prevented delta and omicron fatalities. Why should we believe this claim? “Because I say so.”
The cumulative death data from COVID-19, reported by the CDC, shows that every state experienced a surge in death corresponding to delta and omicron, just at different times. States with high vaccination rates had these waves; states with low vaccination rates had these waves. Instead of vaccination rates, population density correlates better with COVID deaths. New York City, a highly vaccinated area, has the highest cumulative COVID death rate, nearly 500 per 100,000 population. Why believe that universal vaccination would have prevented deaths? “Because I say so.”
The CDC Heat Map plots case rates and vaccination rates. If vaccination prevents COVID, then the map should be colored red (high cases in areas of low vaccination) and green (low cases in areas of high vaccination). Instead, there is lots of purple—high numbers of COVID cases in highly vaccinated regions of the country. If COVID cases are highest in the most vaccinated regions of the country, why should we believe that universal vaccination would have saved lives? “Because I say so.”
The NPR article goes on to perpetuate a pejorative stereotype. Vaccination rates are lower in red states—read “Trump voters”—implying that Trump voters are just not intelligent enough get vaccinated. The article suggests that people from blue states are more trusting of government, as if that is desirable. It goes on to blame Republican-led states because they “underused other pandemic-fighting tools, such as mask and social distancing requirements,” ignoring that these pandemic-fighting tools were first implemented by the Trump administration. Furthermore, today’s CDC COVID Data tracker shows COVID-19 Community levels are highest in the Northeast—blue states. So why should we believe this red state/blue state narrative? “Because I say so.”
The article commends Massachusetts, a highly vaccinated blue state, for its low rate of vaccine-preventable deaths. However, the CDC’s data tracker shows an interesting and unexplained anomaly. Miraculously, on March 14 nearly 4,000 fewer individuals had died from COVID in Massachusetts than were reported the day before.

MASSACHUSETTS
March 13, 2022: Total deaths 23,751, Death rate per 100k 345
March 14, 2022: Total deaths 19,981, Death rate per 100k 290
FLORIDA
March 13, 2022: Total deaths 73,152, Death rate per 100k 341
March 14, 2022: Total deaths 73,194, Death rate per 100k 341On March 13, the Massachusetts death rate was higher than Florida. On March 14, the Massachusetts death rate was lower than Florida. Why the forensic audit and recount of the Massachusetts data, the result of which smoothed out a surge in the state’s reported COVID deaths? Maybe the facts did not fit the narrative. But we should believe the narrative anyway, “Because I say so.”
Who are you and where did you publish your data?
Researchers at Brown and Microsoft AI Health provided this data analysis, but not in a peer reviewed medical journal. Instead, the data was “shared exclusively with NPR.”
Let me get this straight. An ivy-league university, a big tech company, and a left leaning news organization are telling us, “Get your vaccination, get your booster, because I say so.”
Not good enough for me. How about you?
- A Pandemic of Fascism
In a recent post, I called those using the pandemic to increase wealth and power fascists. Fascism is a charged word, but I used it deliberately. Simply stated, fascism is the alliance between business and government to give wealth to the former and power to the latter. The cost of fascism is borne by common citizens who pay with their money and freedom.
The word “fascism” has become a pejorative used to shut down debate by conjuring images of swastikas, concentration camps, and sieg-heil salutes. True, a notorious example of fascism was its use by National Socialists in Germany to consolidate power and wealth around a monolithic cultural and racial ideal. Nazism’s twisted utopian goals have been used by American leftists to brand their opposition as fascists, destroying the true meaning of the word.
Fascism is not a defining characteristic of the political right or the political left. It is not even a tendency of one political party more than another. It is a tendency of any politician who becomes intoxicated by power. Realizing that a position in government can be stealthily misused for selfish ends, corrupt individuals entrusted to safeguard our interests easily find accomplices ready to deal for sure profits. It is an unforgivable, treasonous violation of sacred honor and duty.
Fascists use a crisis to create panic, then demonize a segment of the population for causing the crisis. By doing so, they trick many into mindless submission. Today’s fascists have perpetuated the pandemic and castigated the unvaccinated, using fear to cover their true agenda. Because they cannot prevail using honest, intellectual arguments, they resort to coercion, bullying, oppression, suppression, and ad hominem attacks. Even violence is permitted if it furthers their cause. There is an inevitable trail of pain and death in the fascists’ wake.
Think that is harsh? First consider that those assuring the safety and efficacy of COVID vaccines are also those with most to gain by vaccine sales. Then look at the 40% increase in death among working aged adults during 2021. Look at the higher all-cause mortality among the vaccinated within Pfizer’s own clinical trial dataset. Look at the thousands of suspicious deaths reported to VEARS. Look at the attempt by FDA to hide Pfizer data from the public. Look at the 13 times higher rate of myocarditis in young men aged 16 to 19 who have taken mRNA vaccine. How do we account for these failures?
Perhaps COVID-19 is so new that the medical-industrial-regulatory complex could not have possibly anticipated these outcomes. Perhaps in haste to bring a savior vaccine to market, they neglected to perform a thorough analysis of the data. But is ignorance or willful neglect among those who claim the ability to interpret science—who claim to be science—acceptable?
Instead, perhaps they were fully aware of all the data and decided that the risks were worth the potential benefit anyway. Decided for you. Decided for you and as many other individuals as there are Americans. This is what fascists do. They decide for you, or rather they decide what is best for themselves and coerce you to comply. Coercion like vaccine mandates, for example.
But weren’t vaccine mandates overturned by the Supreme Court? Not quite. The CMS mandate is still force. Think about how it works.
CMS refuses to pay for healthcare services rendered to Medicare subscribers unless most members of the provider organization are vaccinated. Sure, some members of the organization can opt out of vaccination, so long as there are not too many of them, and so long as it is for a medical condition or religious objection. “I don’t want the increased risk of myocarditis and death” is not an acceptable reason to decline the vaccine, the very vaccine which says in its factsheet, “The recipient or their caregiver has the option to accept or refuse Pfizer-BioNTech COVID-19 Vaccine.” Some option, if you have spent the last 30 years of your life in education and training to be a neurosurgeon, and the alternative is unemployment. That cognitive dissonance does not bother fascists. What bothers them is precise use of language.
Nazis were masters of language distortion. Sonderbehandlung (“special treatment”) meant execution, and die Endlösung (“final solution”) meant extermination of all Untermench (“sub-humans”). These terms facilitated polite conversation about horrific crimes at genteel dinner parties, while veiling a threatening sub-text—any individual who stands against fascist institutions can become an Untermench subject to Sonderbehandlung.
Today’s fascists use a similar technique. The label “science” is applied to any flimsy hypothesis that supports their agenda, while opposing yet equally plausible ideas are discarded for lack of “clinical evidence.” They continue to insist, for example, on the zoonotic origin of SARS-CoV-2, dismissing as conspiracy the lab-leak theory or any possible connection to bioweapons research. They change the meaning of words like “vaccine” to suit their ends. “Safe and effective” really means “the issue is settled; stop analyzing the data.” The list is endless. Even the word “fascism” has been distorted, leaving us without language to describe what is happening. Once fascism takes hold, it goes viral, spiraling exponentially in a positive feedback loop. It is insidious. It is infectious.
Although the COVID pandemic has subsided, a Pandemic of Fascism remains. It is a virus, and it is raging across the globe. We need inoculations.
Fascism is a tool to consolidate power, transfer wealth, and reduce liberty. Like SARS-CoV-2, it will never be totally eradicated. It has lingered in our culture for eons. But it must be minimized. Like SARS-CoV-2, fascism must be beaten back to smoldering endemic levels.
Since fascism abhors individual liberty, fairness, honesty, clarity, and diversity, these must be our highest values. They cannot be compromised, not even a little. To recover from this instance of fascism, we cannot let our language be corrupted by Newspeak.
Challenge all assumptions. Take nothing for granted.
- Novavax Uses Magician’s Tricks in Vaccine Study
My last blog described a phase 3 clinical trial for Novavax vaccine published in the New England Journal of Medicine. Like a master stage magician, this study uses distraction, illusion, and manipulation to support its conclusions. In this blog, I will blow away some of the smoke and expose the fraud.
For example, the authors report that all-cause mortality among trial participants is “balanced”—a word probably selected for its positive connotation. But in a vaccine study, balanced all-cause mortality is not desirable. An effective vaccine prevents people from dying from disease, and a safe vaccine does not cause death from vaccine complications. Instead of balance, a reduction in all-cause mortality in a large study population supports the claim of “safe and effective” vaccine. When all-cause mortality is balanced, the vaccine is either ineffective, unsafe, or both. Yet the authors leave the reader with the illusion that “balanced” all-cause mortality is a good thing.
The study concludes that the vaccine is effective. While the data shows Novavax vaccine reduced SARS-CoV-2 infections, most of the infections prevented were mild. The vaccine provided the best protection against the original strain, a strain that is no longer a threat. It prevented “moderate-severe COVID” in a tiny fraction of participants, and it saved no lives. Does that make it effective?
To answer that question, we must examine the other side of the equation. We must ask whether these potential benefits are worth the cost of taking the vaccine. Cost is measured in adverse effects.
Nearly 80% of the vaccinated, four times more than control, experienced adverse effects. Although the reported adverse effects were mild, the monitoring period averaged only two months.
Safety cannot be proven in two months. Because of the law of delayed consequences, observations over years, even decades, are needed to assure a substance is safe for injection. It took generations to recognize the harmful effects of diethylstilbestrol, a synthetic hormone. Yet this study eliminated the possibility of finding serious long-term vaccine complications by eliminating the control group after 3-4 months.
Does this vaccine cause serious consequences 6 months after vaccination? Is all-cause mortality higher in the vaccinated after a year? We will never know because the researchers vaccinated the control group. The study is corrupted. The “A/B” test is now an “A/A” test.
Then, like a great magician, the authors substitute fake science for real science by stating that “hazard models have been proposed for subsequent analyses.”
The proposal to monitor for long term ill-effects with a “hazard model” mocks the clinical trial process. If actual observation of the actual response to actual vaccines in actual human beings over time can be replaced by computer models, why ever bother with clinical trials? Clinical trials are messy, expensive, and painful. Sometimes they flop. Yet clinical trials necessary to establish knowledge. They cannot be replaced by “hazard models.”
This is not just bad science; this is anti-science. Science requires strict adherence to the scientific method. Anything else is wishful fantasy. Or worse—a deliberate deception.
We have seen these tricks before. Eliminating control groups, hiding adverse findings, covering contradictory evidence with high gloss rhetoric, and cherry-picking data characterized Pfizer’s authorization studies. These ruses are eloquently detailed by Robert Kennedy, Jr., in his book The Real Anthony Fauci.
I am not saying that Novavax is a bad vaccine. Maybe an alternative to mRNA is a good thing, and maybe some individuals could benefit from this vaccine. Since the data is incomplete, I cannot say. What I can say is that this study about the Novavax vaccine is dishonest, yet it forms the foundation of Novavax’s EUA application.
And why is FDA considering an emergency use authorization for a new vaccine so late in the game? Clearly, it is time to end the emergency. We need to wind up emergency use authorizations. EUA products should be licensed or discarded. We do not need another EUA vaccine.
Maybe the FDA is considering EUA for “Novavax COVID-19 Vaccine, Adjuvanted” because it is the first COVID vaccine to show feasibility as a combination vaccine with flu. Perhaps this was part of the game all along.
One more thing. Novavax inadvertently debunked the claim that vaccination-induced immunity is superior to disease-induced immunity. The “Novavax COVID-19 Vaccine, Adjuvanted” uses a proprietary protein “Matrix-M,” to present spike protein because it is thought to better resemble virus than other vaccines. According to a company press release, “This arrangement mimics nature, helping your immune system recognize that target protein from different angles—the same way that your immune system would see the details of a real pathogen.”
Until now, we have been told that the immune effects of the real virus are insufficient. We must have spike protein coating our own cells—the proposed mechanism of mRNA vaccines—to stimulate effective immunity, even after infection by real virus. Novavax differentiates its vaccine from mRNA by its ability to mimic a “real pathogen,” implying that real pathogens stimulate the best immunity. Of course, this was the dogma of medical science for eons, until 2020 when the buildup to mRNA vaccine release required a new theory of immunology.
Thank you, Novavax, for setting us straight on this point.
- Control Group Eliminated in Study Funded by Vaccine Maker Novavax
On June 7, FDA’s Vaccines and Related Biological Products Advisory Committee will discuss an EUA request for a COVID-19 vaccine manufactured by Novavax. If the EUA is granted, Novavax will become the fourth vaccine maker permitted to distribute vaccine in the United States.
The “Novavax COVID-19 Vaccine, Adjuvanted” (aka NVX-CoV2373) claims to be different from any other vaccine on the market. It’s not mRNA, and therefore, not gene therapy. Instead, it’s a “nanoparticle” covered in spike protein. The nanoparticle, Novavax’s proprietary protein “Matrix-M,” is thought to better resemble virus than current vaccines. According to a company press release, “This arrangement mimics nature, helping your immune system recognize that target protein from different angles—the same way that your immune system would see the details of a real pathogen.”
A study recently published in the New England Journal of Medicine, together with its supplementary appendix, presents results of a U.S. phase 3 clinical trial for Novavax vaccine conducted by dividing 25,000 participants into two groups. One group received the full two-shot vaccine series, and the other group received two placebo injections.
To determine vaccine efficacy, participants were tested for SARS-CoV-2 infection after receiving vaccine or placebo. Subsequent infection was identified in 77 individuals; most of these were in the placebo group. Only 14 of these infections were considered “moderate-severe COVID,” and all of these were in the placebo group. All infected patients recovered. There were no deaths attributed to COVID in the study.
To study vaccine safety, the researchers solicited reports of adverse effects from participants. Adverse effects were experienced by nearly 80% of vaccine recipients, four times the rate of placebo. Most of these adverse events were mild. The report claims that Novavax is not associated with the types of complications associated with other COVID vaccines:
“No episodes of anaphylaxis, no evidence of vaccine-associated enhanced Covid-19, and no events that triggered prespecified pause rules were observed. No episodes of the Guillain–Barré syndrome and no imbalance in myocarditis or pericarditis or in vaccine-induced immune thrombosis with thrombocytopenia were observed during the relatively short safety follow-up period reported here.”
How short was that safety follow up period? A mean of two months.
Despite the promise to continue the safety review for 24 months, the authors admit:
“We implemented a blinded crossover approximately 3 to 4 months after the first vaccination series to allow all trial participants to receive NVX-CoV2373, after vaccine efficacy and required safety had been established and reviewed by the data and safety monitoring board.”
This crossover hides any potential long term adverse effects in the control group by eliminating the control group. To make up for this deficiency, “hazard models have been proposed for subsequent analyses.”
The authors then conclude “NVX-CoV2373 was safe and effective for the prevention of Covid-19.”
The study fails to report an honest cost-benefit analysis. Although the study legitimately claims Novavax reduces susceptibility to a mild disease, it ignores data showing that cost of this reduction is the likelihood of short-term adverse effects, and it erases the possibility of finding long-term adverse effects which may be more serious than any benefit of taking the vaccine.
Oh, one more thing. Guess who is first on the list of supporters funding this study? Novavax.
Surprised? Me neither.
- FDA Limits Janssen EUA
The vaccine landscape changed today. To keep you up to date, here is a summary of changes and a new vaccine chart.
New Factsheets for Healthcare Providers have been issued for Pfizer Purple, Gray, and Orange vaccines. The Pfizer family of vaccines are now authorized for two booster doses, the first of which may be given five months after a primary series in individuals 12 and older, and a second may be given four months after the first booster in individuals 50 and older and in individuals 12 and older with “certain immunodeficiencies” defined in the authorization letter as individuals “who have undergone solid organ transplantation, or who are diagnosed with conditions that are considered to have an equivalent level of immunocompromise.” Pfizer Orange is authorized for a third shot in the primary series for individuals 5 through 11 with the same “certain immunodeficiencies,” but not for boosters. Each of these new factsheets (Purple, page 44; Gray, page 41; Orange, page 33) contain a statement I don’t remember seeing before: “Available data on Pfizer-BioNTech COVID-19 Vaccine administered to pregnant women are insufficient to inform vaccine-associated risks in pregnancy.” Show this to your OB if you are pressured to get a vaccine while pregnant. I am unable to explain why CDC still recommends COVID vaccines for “people who are pregnant, breastfeeding, trying to get pregnant now, or might become pregnant in the future.” These authorizations also extend the vaccine expiration dates. COMIRNATY, the only vaccine approved for individuals 16 and older, is still unavailable in the United States.
Moderna vaccines now have a complicated color scheme. The authorized Moderna COVID-19 Vaccine, and the approved SPIKEVAX (COVID-19 Vaccine, mRNA) both have red caps with a light-blue border. These are given in full dose (0.5 ml) for primary series and half dose (0.25 ml) for booster. The Moderna COVID-19 Vaccine also comes in a booster-only half-strength vial recognized by its dark blue cap with purple border given as a full dose (0.5 ml). Presumably, this is to cut down on confusion between the primary series and booster dosing, but it has resulted in a very complicated updated authorization letter. Moderna first boosters are authorized five months after the primary series for a first booster in individuals 18 and older, and four months later as a second boosters for individuals 50 and older and in individuals 18 and older with “certain immunodeficiencies,” defined the same as for Pfizer. On page 29 of the Blue/Purple factsheet is the same warning issued for Pfizer: “Available data on Moderna COVID-19 Vaccine administered to pregnant women are insufficient to inform vaccine-associated risks in pregnancy.” Moderna boosters may be preferred by your doctor since they are thought to produce the encouraged highest antibody response; I’m not convinced that is a good thing. SPIKEVAX, Moderna’s approved vaccine, is still unavailable in the United States.
FDA has limited its authorization for the Johnson and Johnsons vaccine. There is a new Factsheet for Healthcare Providers that starts with a prominent warning about its blood clot complication. Page 26 contains the familiar pregnancy warning: “Available data on Janssen COVID-19 Vaccine administered to pregnant women are insufficient to inform vaccine-associated risks in pregnancy.” CDC recommends Moderna’s and Pfizer’s family of vaccines over Janssen. The vaccine expiration dates have been extended.

Vaccine Chart, Revised May 5, 2022. The FDA has announced a tentative schedule for it’s Vaccines and Related Biological Products Advisory Committee (VRBPAC). On June 7, the committee will consider an EUA request for the Noravax COVID-19 Vaccine. It will be live-streamed on FDA’s YouTube channel.
- End Games
The pandemic is over. Sure, a few hot spots remain, and SARS-CoV-2 continues to smolder as variants of the original virus, but this is our post-pandemic world. COVID will never be eradicated; there will always be endemic disease where there are human communities. But the worldwide pandemic, the catalyst for the “emergency”, has passed. This emergency created an alliance between power hungry authoritarians and money hungry profiteers, resulting in a loss of individual freedom and massive wealth redistribution.
This alliance has not ended with the COVID emergency. Politicians and the industrialists will continue to conspire to secure the profits and power usurped during the past two years, and they will do this by playing games. Get ready for the end games.
Many of these games will be played with emergency use authorizations (EUAs). Medical devices and therapies developed during the pandemic continue to be available under EUA for as long as HHS Secretary determines that there is an emergency warranting use of unapproved products. On April 12, 2022, Xavier Becerra renewed the declaration, extending the emergency into July. But does anyone think that a true emergency still exists? As COVID restrictions are lifted, the only reason for the continued “emergency” is to prolong the availability of these profitable medical devices and therapies.
Manufacturers would rather operate under EUA than under FDA license because of relaxed manufacturing standards and minimal product liability, but the beneficiaries of the emergency know this state cannot not last forever. They intend to ride the EUAs until the end, then jump over to FDA approval at the last possible moment so their profits continue after the lifting of the emergency declaration.
These end games are baked into the pre-pandemic language governing EUAs. The Secretary of HHS is required to give adequate warning before terminating an emergency so that manufacturers may dispose of their outstanding inventory. Last month, FDA issued draft language outlining a transition plan from EUA to approval for medical devices, including PPE equipment and diagnostic tests. Expect similar plans for drugs and vaccines.
Pfizer and Moderna have already pocketed approvals for COMIRNATY and SPIKEVAX without bringing these products to market. Once the emergency ends, these vaccines will magically materialize. But before the state of emergency is lifted, vaccines will be approved for all age groups, as will perpetual and unlimited boosters.
The same will be true for other expensive, patentable COVID drugs such as Evusheld and bebtelovimab, drugs designed for pre-exposure and early treatment and now only available by EUA. Before the emergency is lifted, there will be a push for FDA approval by the same forces that conspire to prevent access to Hydroxychloroquine and Ivermectin which have been used for the same purposes. The existence of these unpatentable drugs should have precluded EUAs for the profitable ones.
Another game is being played with tests. Early in the pandemic, the CDC quietly changed the definition of cases to mean a positive diagnostic test regardless of symptoms. This change drives up the case rate numerator without changing the denominator. These inflated test results will be used to prolong the emergency declaration for as long as possible, stretching the advantageous EUA business environment. With few exceptions, SARS-CoV-2 tests are available by EUA, but these will be quickly approved before emergency is lifted, since direct viral tests are useful to perpetuate fear in a sensitized population.
By the way, do not expect antibody tests to be approved any time soon. Antibody tests should be the gold standard for assessing immune status—better than vaccination history, better than disease history. But these tests are still shockingly primitive. No interpretative standards have been developed, and few careful serologic studies have been undertaken. And no wonder. The potential clarity of antibody tests benefit neither the profiteers nor the authoritarians.
And what do the authoritarians get by playing these games with the profiteers? Power. In exchange for their friction-free money machines, businesses have facilitated the authoritarian’s assault on civil liberties. Businesses use a variety of techniques to steal liberties from individuals. Some of these liberties are surrendered freely by appeals to conscience and duty. Other liberties are taken by coercion. But when force is required, businesses provide the muscle. Hospitals fire employees that refuse to comply with the CMS vaccine mandate. Airlines enforced the CDC transit mask mandate, and may do so again. Neither mandate is supported by evidence.
The current powerful alliance of big business and big government fulfills the criteria of fascism. Americans have been here before. To overturn this instance of fascism, we need coalitions of citizens committed to truth and individual liberty. Our greatest hope is rekindling the American Spirit.
- Where Is the Evidence That Flu Vaccines Save Lives?
The prevailing presumption that flu vaccines save lives is based on faith in policymakers who are trusted to safeguard our health. There is little evidence that this presumption is true.
Viruses are classified according to their size, shape, and the type of genetic material they contain. Influenza viruses are Orthomyxoviruses, a family unrelated to Coronavirus. Of the four known types of influenza viruses, infections by Flu A and Flu B cause most illness in humans. Flu A is subtyped according to the type of H and N proteins on the viral surface. Flu A(H3N2) and Flu A(H1N1) have been prevalent in recent years, but others have been significant in the past. Just like SARS-CoV-2, influenza viruses mutate rapidly, so that different variants circulate each season.
Where is the evidence that flu vaccines save lives? The question is more difficult to answer than it seems at first glance. The way that flu mortality is calculated and tracked has changed over the last hundred years. Criteria for diagnosis of influenza vary, and the treatment of flu and its comorbidities has changed with time. Vaccine formulations, strategies, and target prediction methods are constantly evolving. These challenges frustrate the impulse to google the answer. But I am going to try.
Using annual population estimates from the U.S. Census Bureau website and flu mortality from the CDC website, I calculated annual flu mortality rates for each of the ten flu seasons prior to the pandemic, and I compared these to flu vaccination rates published by the CDC for the same period (table 1). I chose these years because of the relatively consistent data reporting during this time. If flu vaccinations save lives, years of high flu mortality should have low vaccination rates, and years of low flu mortality should have high vaccination rates.
I found that if vaccination impacts flu mortality, it is only one of several factors and probably not the most important. The data shows an inverse correlation between vaccination rates and flu mortality for only six years (top chart, blue points, correlation coefficient = 99.5%), but adding the pesty outlier years to the data set results in poor linearity for the decade (correlation coefficient = 23.6%). In three of these outliers, the mortality is lower than predicted by the vaccination rate (green points), but in one year, the mortality is higher than predicted by vaccination rate (red point). The 2013-14 Flu season had the highest mortality rate (16.4 deaths/100,000 population) but a middling vaccination rate (53.7%, Mean 54.4%, Standard Deviation 3.1%).
More troubling is the poor relationship between vaccination rates and flu deaths among the elderly (table 2). Individuals aged 65 and older are most susceptible to flu complications, yet it is hard to find any correlation between vaccination rates in these individuals and flu mortality (bottom chart, correlation coefficient = 36.8%). While vaccination rates among the elderly were stable during the 10 years prior to pandemic, (60-70%, mean 65.6%), mortality rates varied wildly, between 22.6 and 100.7 deaths/100,000 population.
A few words of caution. Drawing conclusions from ten data points is dangerous. My data does not include the vaccination status of those who died from flu; maybe that information would show much higher mortality in those who did not receive vaccine. But similarly, I have not considered the mortality rates of those who survived flu infections from previous seasons. Perhaps natural flu immunity is more durable and protective than vaccine immunity. This idea is supported by the surprising finding of negative excess mortality among elderly individuals during the 1918 “Spanish” influenza pandemic. The same questions that can be asked about natural and vaccine-induced immunity for COVID-19 can be asked about influenza.
I am not the first person to question the efficacy of flu vaccines, especially among the elderly. According to studies often cited by policymakers, vaccination results in an astronomical reduction in flu mortality. But not everyone agrees. Analytic flaws resulting from confounding evidence and bias muddle these conclusions. Tom Jefferson, an epidemiologist and editor of the Cochrane Acute Respiratory Infections Group, says plainly, “The large gap between policy and what the data tell us is surprising.”
Flu mortality has declined since 1900; however, the first part of this decline cannot be attributed to flu vaccines since they were not used before 1940. Even after vaccines were widely available, they were unlikely the explanation for declining flu mortality. A 2005 study funded by National Vaccine Program Office stated bluntly, “We could not correlate increasing vaccination coverage after 1980 with declining mortality rates in any age group.”
While overall flu mortality has declined since 1900, the proportion of deaths among those 65 years and older has increased. Could this change be due to aggressive vaccination policies which have deprived young people of the opportunity to develop natural flu immunity, pushing their infections into later life when they are more vulnerable? Is our financially conflicted health care industry deliberately creating pandemic paranoia by its annual warning of a resurgent Flu Apocalypse?
Of course, the absence of supporting data does not prove a proposition false. I am not saying that flu vaccines do not save lives; they might. But there is little compelling evidence generated by well-designed, bias-free, placebo-controlled studies. The presumption that flu vaccines save lives is based on faith, not science.
Public officials paid to establish health policy have violated our trust, misusing the vaccine paradigm to generate windfall profits for the pharmaceutical industry. From now on we demand hard data instead of platitudes.
- Post-Pandemic Stress Disorder
Seasonal upper respiratory infections are not new, but we are responding with a new emotion—fear. We have been traumatized by the pandemic, and that has created a unique form of post-traumatic stress disorder. Some of us will need treatment, but most of us can snap out of it. How and when we conquer our fear will determine the world we give our children.
The normal brain is not like a security camera. Instead of recording activity, sensations, and body conditions in a continuous moment-to-moment reel, typical memories are collections of patterns and associations. Gaps between significant events are cut from our recollection. A birdwatcher is more likely to remember rare species observed rather than the order or times birds are seen during an outing.
Intense emotions change the way memories are made. These emotions need not be unpleasant; it is the intensity of feelings that matters. During these moments, memories are seared into the brain in vivid detail. It is more than what happened; the emotions of the experience become part of the memories.
Trauma is the body’s response to imminent danger. The threat can be against your status, your self-image, or your very life. Trauma does not require real danger; the perception of danger is enough. If the threat seems real and the emotions intense, a traumatic memory can result.
Trauma changes the mind. We have a primitive impulse to protect ourselves from harm. When we encounter a situation that reminds of a past threat, we instinctively defend ourselves using the acute stress response—fight, flight, freeze or fawn. Individuals triggered in this way can be combative, avoidant, catatonic, or irrationally conciliatory. First recognized in World War I veterans as “shell shock,” this is the basis for our modern understanding of post-traumatic stress disorder.
Collective trauma can change a generation. Those who lived through the Great Depression endured a period of inescapable poverty. Shantytowns sprang up as the number of destitute increased. Those who survived this period abhor waste, hoarding items of little value because they fear running out. Traumatized by their collective experience, many who grew up during this time could never shake their fear, and this fear limited their future productivity. Known as the Silent Generation, this is the only generation of Americans to not produce a President.
Trauma causes trauma. The response to trauma by one person can cause a trauma in another person, creating a deteriorating spiral of disfunction. For example, patterns of violence are often observed in families, passed from one generation to the next. The traumatized may vow to never allow themselves to be threatened again, resulting in a display of power that threatens others, and the cycle perpetuates. This is what the pandemic has done to us.
COVID-19 has been traumatic. We survivors have lived through a mortal threat. Most of us know someone—probably someone close—that succumbed to COVID-19. Deaths associated with COVID-19 are still happening today, but not nearly at the rates of 2020. We sought protection in vaccines and expensive new drugs, and we wanted to believe they could save us from this deadly threat. Now our fear is exploited by unscrupulous leaders who tell us it will work only if we all believe. Just as the virus posed a threat to our lives, the response by those in power poses a threat to our liberty. Those who do not comply with the plan of protection do not deserve the fundamental rights of a human being. They are not human—they are other than human.
How do we break this cycle?
First, we must put the threat in context. Although a threat still exists, we have advanced in the fight against COVID-19. Deaths from COVID-pneumonia this winter are comparable to deaths from community acquired pneumonia during pre-pandemic years.
Using 2019 US Census Bureau data and the weekly COVID mortality data for December 25, 2021 published on the CDC’s COVID Data Tracker, I calculate an overall annualized COVID mortality rate of 7.5 per 100,000 population, which is higher than the rate published on CDC’s website. During the mild flu season of 2011-12, the annualized flu mortality per 100,000 population was 3.8, about half the current rate of COVID mortality. But during the severe flu seasons of 2014-15 and 2017-18, the annualized mortality per 100,000 population was over 15, double the current rate of COVID mortality. The current COVID-19 mortality rate is less than flu in a bad year.
Second, we must put the vaccine debate in context. A recent MMWR report shows that individuals who were both unvaccinated and uninfected during the Delta wave had a higher incidence of hospitalization. Vaccination keeps people out of the hospital, but at what cost?
A critical analysis of Pfizer’s FDA submission data shows that vaccination is associated with two extra cardiac deaths for every COVID death avoided. The same data shows that all-cause mortality is greater among those who received vaccine (15/22,000) than placebo (14/22,000). By the way, if you want to review this data for yourself, search for Table S4 in the supplementary information. Table S4 is referenced in the article, but it is not published there. To paraphrase the Wizard, you are to pay no attention to the data behind the curtain.
Finally, we must let go of our fear. Easy to say, hard to do. Trauma has a way of working fear into your body; you cannot just eliminate it with the strength of your will. Everyone’s specific path will be different. Those most severely affected by post-pandemic stress disorder will need professional treatment; these individuals deserve our compassion. But generally, we let go of unrealistic fears by realizing the monster is not scarier than other risks we face daily.
One way to do this is to give the fear a name—“name it to tame it.” Calling out what scares us is a way to release unrealistic fears. For example, COVID has caused many of us to be afraid of people who have different ideas about the pandemic, but when we realize this is a fear of diversity, it may be easier to let that fear go.
We cannot expect everyone will choose the same course of action, but we must treat each other with respect anyway. The same MMWR report that shows vaccination keeps people out of the hospital also shows that those with natural immunity are about half as likely to be hospitalized as those with vaccine-induced immunity alone. Does that mean we should fear those who have avoided SARS-CoV-2 infection? Of course not. But neither should we fear the unvaccinated or unmasked. Fear makes us vulnerable to manipulation designed to perpetuate the pandemic. We must stand fearlessly against irrational one-size-fits-all policies.
The pain of the pandemic is present still. The pandemic has taken lives. Our pandemic response is breaking lives and destroying livelihoods. Some of you may no longer fear COVID-19, but you still fear losing your job, losing access to medical care, or being ostracized for your beliefs. We cannot let trauma trap us in pandemic forever. What we do now determines the type of life we pass to the next generation.
We love our children and desire to bequeath a better world to them. We cannot make them spend their lives cleaning up this mess. For the sake of our children, we must allow our traumatic memories to fade.
- Moderna’s Spikevax Approval Echoes Comirnaty
On Monday the FDA approved Spikevax, the second licensed COVID-19 vaccine. But Spikevax will be as elusive as Comirnaty. Even though the FDA press release makes it sound like Moderna is simply changing the name of its COVID-19 Vaccine to Spikevax, Moderna COVID-19 Vaccine will continue to be available under EUA just like Pfizer-BioNTech COVID-19 Vaccines. As with Pfizer, FDA has approved a phantom vaccine while using EUA to shield Moderna from product liability. Instead of protecting Americans, the FDA is double-dealing deceptively to benefit a large pharmaceutical company.
FDA issued two letters on January 31, 2022, both addressed to Michelle Olsen of ModernaTX, Inc. The first letter permits the company to market its COVID-19 vaccine under the label SPIKEVAX. FDA took this action without a referral to the Vaccines and Related Biological Products Advisory Committee because Moderna’s Biologics License Application (BLA) “did not raise concerns or controversial issues that would have benefitted from an advisory committee discussion.” Which is not the same as saying the BLA does not raise concerns or controversial issues.
Potential concerns and controversial issues are detailed later in the letter as “Postmarketing Requirements/Commitments.” These include studies to address the effect of the vaccine on children, due in 2024, and studies to determine the risk of myocarditis, due between June 2023 and October 2028. The results of required studies on the effect of the vaccine on pregnancy will not be known until June 2024, but the product can be distributed just as soon as Moderna receives “a notification of release from the Director, Center for Biologics Evaluation and Research.”
The second letter reaffirms the Emergency Use Authorization for Moderna COVID-19 Vaccine. This letter offers flimsy reasons for the persistence of the EUA. For example, the letter states that
Although SPIKEVAX (COVID-19 Vaccine, mRNA) and Comirnaty (COVID-19 Vaccine, mRNA) are approved to prevent COVID-19 in certain individuals within the scope of the Moderna COVID-19 Vaccine authorization, there is not sufficient approved vaccine available for distribution to this population in its entirety at the time of reissuance of this EUA.
Footnote 11Of course, there would be sufficient approved vaccine if FDA required Moderna to relabel existing inventory as “Spikevax.” This option is not addressed in the letter.
The letter goes on to say that the scope of the license is a subset of the scope of the EUA, and that the EUA must continue so that vaccine is available in unapproved situations. Of course, those situations could be addressed in an EUA that excludes the licensed situations, but that option is not considered in the letter.
Finally, in language that seems to have been boilerplate from the Pfizer-BioNTech EUA, the FDA will allow Moderna COVID-19 vaccine to be administered to individuals 18 years under EUA because “there remains, however, a significant amount of Moderna COVID-19 Vaccine that was manufactured and labeled in accordance with this emergency use authorization.” Does that mean that Moderna will stop manufacturing the EUA version of its vaccine and just consume inventory? I doubt it.
According to its package insert, Spikevax is approved for adults 18 years and older as a two dose primary series. However, like Comirnaty and Pfizer-BioNTech Purple, the revised Vaccine Information Fact Sheet about Spikevax and the Moderna COVID-19 Vaccine permits Spikevax to be used interchangeably with Moderna COVID-19 Vaccine.
So now our vaccine chart looks like this:

Within a vaccine landscape that is more complicated than ever, we still do not have a licensed COVID-19 vaccine for Americans.
- Free Tests We Cannot Afford
A new crisis has been spawned by the pandemic. This crisis was announced by the President in December, and it will consume more and more bandwidth in coming months. It is the crisis of testing. This is a fabricated crisis, unrelated to people’s health. This crisis is a distraction designed to perpetuate the pandemic so that more of your wealth can be transferred from public coffers into the pockets of special interests.
On December 21, in the same speech that introduced the testing crisis, the President announced an initiative to make 500 million free tests available to Americans. These tests can be ordered “free of charge” at covidtests.gov, and they will delivered to your home by the US postal service. Furthermore, the government has “incentivized” insurance companies to reimburse Americans for over-the-counter tests, up to eight tests per covered individual per month.
As Omicron burns through the country, it’s time for a dose of common sense. Omicron is mild. With over-the-counter medications and the advice of Front-Line doctors, most people can recover at home, without a test.
Many people think that a negative test means that you cannot infect others, but that is not the case. PCR tests have issues, but over-the-counter tests are antigen tests, and antigen tests are notoriously unreliable. Using manufacturers’ submission data, over-the-counter tests have average sensitivity confidence intervals of near 70%, meaning that up to 30% infected people will have a negative test. Results are influenced by timing and technique. Test too early, and the confidence intervals can drop below 40%. A negative test does not mean you cannot spread disease, and a positive test does not mean you will spread the disease. Using test results to control social, educational, and business interactions will fail to stop the spread of the virus. Relying on test results to determine who is sick and who is not is dangerous.
So why the push for testing? Two reasons. It’s a boondoggle, and it perpetuates the emergency.
“Free tests” for all Americans are not really free to all Americans. The government buys them with taxpayer dollars from companies that have little incentive to produce quality tests. This is because the tests are available by EUA which eliminates the manufacturer’s liability. There is no consumer protection for shoddy work, no matter how egregious. Even more, these companies have a governmental market guarantee. With the promise of four free tests per address, manufacturing test kits is the same as printing money.
But even worse is how indiscriminate testing adds to pandemic panic. Every positive test raises the CDC’s case count, and rising cases fuel the pandemic, keeping the emergency active. It should be clear to everyone that the emergency is over. We have treatments, we have ventilators, we have vaccines, we have hospital beds. The original emergency was two weeks to flatten the curve. We’ve reached a status quo. We may not like where we are, but here we are anyway. It is no longer an emergency.
It is time we take down our emergency provisions and restore power to the people. Stop obsessing, stop naming, stop testing indiscriminately. Everyone knows when they are well and when they are under the weather. It is time to use common sense about our new common cold.
We know what to do when we have cold symptoms. Stay home from work, stay away from vulnerable family and friends, and take the vitamins and therapeutics recommended by Front-Line doctors. Go to the emergency room if you have trouble breathing, if you do not get better, or if something feels different than a common cold.
Fight corruption and help end the pandemic. Test as directed by your doctor, not by your government.
- Follow the Money
This is the story of how conflicts of interest have compromised the integrity of our government’s public health policies, favoring special interests instead of the best interest of Americans.
When the pandemic first washed over us, it knocked many of us off our feet. Policymakers shot-gunned solutions in reaction to terrifying mortality rates, especially among the elderly. We needed treatments, ventilators, hospital beds, and vaccines; we needed them fast. We were in no position to bargain.
This chaos created opportunity. Handsome rewards were promised to those offering remedies for the unthinkable. Quoting Robert F. Kennedy, Jr., “Nothing sells vaccine like panic.” This has been especially true of Pfizer, the manufacturer of the Pfizer-BioNTech COVID-19 Vaccine.
Who pays for Pfizer vaccines? Not the vaccine recipients. At least not directly. According to the Wall Street Journal, the U.S. Government pays Pfizer $24 for every vaccine administered against an estimated cost of $1.20, a profit of at least $22 per shot. Every first dose, every second dose, every third dose to the immunocompromised, every booster, every accidental dose to someone previously vaccinated—all generate $22 in profit. OSHA mandates, CMS mandates, and reductions in minimum vaccination and booster ages increase the target market, sales, and profits.
The result is a windfall for Pfizer. According to its third quarter SEC filings, Pfizer’s YTD revenue as of October 3 2021, soared to $57.7 billion, nearly doubling its $30.2 billion revenue for the same period in 2020. At the same time, Pfizer’s net income more than doubled, up 224% from $8.3 billion to $18.6 billion through the third quarters of these years, working out to $3.32 per share of common stock.
The same government that pays for the vaccines regulates the product and mandates its use. This creates a conflict of interest on its face. Furthermore, no one involved in assuring the “safety and efficacy” of vaccines has disclosed a potential conflict and recused themselves from participation in the debate, acceptance, and approval of Pfizer’s vaccines and its reimbursement system. Are we to believe that not one has a financial interest in Pfizer?
If we disrupt their money machine, companies like Pfizer threaten us with the loss of wonder drugs. Research and development costs money, they tell us, and many drugs never make it to market. Pills have a high price because pharmaceutical companies must recoup these costs. Don’t mess with us, they say, or you will lose the gumball machines that dispense the new and improved drugs keeping you alive and happy.
Husain Lalani, MD, MPH, a proponent of universal vaccination to eradicate SARS-CoV-2, together with colleagues Jerry Avorn, MD, and Aaron Kesselheim, MD, published a recent article in Clinical Pharmacology and Therapeutics which demonstrates that COVID-19 vaccines are the result of “decades-long taxpayer investments” prior to the pandemic. Then we funded the clinical trials necessary to bring product to market. According to Dr. Lalani, “in total, over $18 billion dollars of US public funds have been invested in 6 [COVID-19] vaccine candidates.” You and I have paid for these vaccines, so why don’t we own them, instead of Pfizer?
Under the guise of altruism, the pharmaceutical industry is robbing the public treasury while gouging its customers. Government subsidies invalidate the industry’s justification for high drug prices. It’s never been about your life and happiness; it’s always been about their bottom line. The cost is spread across the population, like a tax. The benefit is concentrated in a few companies and their shareholders, like special interest fraud.
The essence of capitalism is to assume risk. Capitalists naturally seek to minimize risks and costs but using power and influence to offload them to the public is corruption. It is easy to see. Just follow the money.
Many see the pandemic as an opportunity to accumulate wealth and consolidate political power. We need to love our freedoms more than we fear the loss of wonder drugs, more than we fear a germ. Americans must stop bickering and start figuring out how to fight greed and evil. The first step is to eliminate corruption. Let’s start with the corruption we can see.
- Doctors Be Doctors
Some physicians are scientists, but most physicians are practitioners like me. There’s a difference. Right now, we need doctors to be doctors.
Scientists study disease and test treatments by applying the scientific method to clinical trial enrollees. The more scientists know about individuals in their study, the more likely that bias creeps in and pollutes the conclusions. That’s why the best clinical trials are large, randomized, double-blinded and placebo controlled. They are focused on populations instead of individuals. Subjects in a clinical trial are part of a science experiment; rather than receiving cutting edge treatment, they may be getting no treatment at all.
The scientific method requires strict discipline. Anecdotal data is anathema to true scientists, to the point that “anecdotal” has become synonymous with “unscientific” and “unreliable.” These words are often used pejoratively to malign the reputation of a report, an observation, or an individual. But it need not be so. Science is not the only path to reliable information.
Practicing doctors use a different method to understand disease and guide treatment. Practitioners look at patients one at a time and tailor treatment individually. The more that physicians know about their patients, the better their treatment results. These doctors watch the outcomes. Treatments that consistently produce better outcomes are favored over those that do not.
The experience of each encounter feeds back into a doctor’s therapeutic approach with other patients. For example, if a patient has a poor outcome after taking a particular drug, the doctor prescribing the drug will be less likely to prescribe it in the future. On the other hand, if a patient has a good outcome after taking a particular drug, the prescribing doctor will be more likely to use it when treating other patients. Communication of these experiences among doctors quickly optimizes treatments.
It is not science, but it is not wrong either. It is more like a search engine algorithm, like A/B market testing, or like crowdsourcing. These are effective methods of finding efficient pathways well known to the technology sector. It is AI, except it is not artificial; it is just intelligence. That is what it means to be a doctor.
Collectively, doctors are a massive learning machine, plowing through data one point at a time. It is not surprising that doctors can find new uses for old drugs. It is not surprising that these old drugs can have long established safety records, even if they are no longer patentable. It is not surprising that repurposed drugs can be effective treatments for COVID-19 despite the absence of supporting clinical trials.
Science is an important tool for understanding reality, but it is not the only way to find truth or effective therapies. Not all medicine is based in science; there is also art in medicine which values anecdote. Over-reliance on science eliminates the opportunity for people to benefit from the power of information collected by practicing doctors, one patient at a time.
Like any tool, science can be abused or manipulated. The integrity of science is the same as the integrity of the people doing science. People who oppose treatments based on the absence of supporting scientific data are bullies, misusing science to get their own way. These science chauvinists have let us down. Worse than that, doctors who have forgotten how to be doctors and who rely exclusively on science have let their patients down.
When all of this is over, when the world turns around, brave doctors will have to rebuild healthcare from scratch, earning public trust again, one patient at a time.
- More Testing Less Freedom
President Biden unveiled a new COVID initiative in a press conference this week. In addition to more COVID vaccinations, he promised more COVID testing. This is a bad idea which will create more fear and less freedom. Testing plays an important role in medical decision making, but indiscriminate testing can lead to harm. To be beneficial, the right test must be selected at the right time for the right reason. Let’s compare Biden’s testing plan against these three pillars of laboratory medicine.
The right test. The President promised free at-home tests. Although his speech was short on details, I think it is safe to assume he is talking about antigen tests which work much like at-home pregnancy tests. Antigen tests are fraught with technical and interpretative challenges, making it difficult to separate signal from noise. The result of increased antigen testing will necessarily be an increase in positive test results, many of which will be false positives. By contrast, PCR tests do a much better job of separating signal from noise. Although PCR test results are often misinterpreted, they have far fewer analytic false positives. President Biden’s plan increases availability of the wrong test.
The right time. There is no test for COVID-19, so the President’s call for increased “COVID” testing is technically incorrect. COVID-19 is a disease caused by SARS-CoV-2 infection. To have COVID-19, you must be infected by SARS-CoV-2 at the same time you have symptoms of a respiratory infection. Symptoms without SARS-CoV-2 infection is not COVID-19; SARS-CoV-2 infection without symptoms is not COVID-19. Why does this semantic detail matter? Because test timing is crucial to the diagnosis of COVID-19.
Test too early and an infectious person may have a negative result. Test too late and a person who is no longer infectious may have a positive result, no matter the quality of the test. This happens with PCR tests and antigen tests alike. Just like there is no morning-after pregnancy test, there is also no morning-after SARS-CoV-2 exposure test. Indiscriminate testing will lead to the wrong people isolating. There will be individuals who consider themselves safe because of a negative test result, and there will be individuals who disengage from society because of a positive test result. Both groups will be wrong because they test at the wrong time.
The right reason. Test results should drive actions; there is no other reason for testing. You should never test for curiosity, because you can, or to confirm a hunch. This is a testing trap that ensnares many of my clinical colleagues. By his call for “more testing,” it appears to have ensnared the President also. Before a test is performed, there must be a clear, distinct plan of action for each possible test outcome. If the actions are the same, the test should not be performed. The indiscriminate testing proposed will be used for the administration’s “vaccinate-or-test” plan. This is the wrong reason.
Vaccinate-or-test. In his press conference, President Biden reiterated his “vaccinate-or-test” plan to control social intercourse. His plan will fail to control viral spread since both of the plan’s foundational assumptions are false. The first assumption is that vaccinated individuals cannot spread infection, but it should be clear to everyone now that this is false. The second assumption is that individuals who test negative for SARS-CoV-2 cannot spread infection, but since the President proposes the wrong tests at the wrong time for the wrong reasons, this assumption is also false.
What will really happen because of the increased indiscriminate testing mandated by the President’s plan?
More Tests Less Freedom. When the wrong test is performed at the wrong time for the wrong reason, the absolute number of positive results will increase. Even though some of these positive results will be false and many will be insignificant, all these results will be counted as COVID “cases.” This is because early in the pandemic, the CDC changed its definition of a COVID-19 “case” from positive test and symptoms to positive test or symptoms. This “case” spike will be raised as a pitchfork to incite fear among Americans, and fearful people are more likely to turn loose of their liberty. Think I’m wrong? Consider this statement made by the President during his press conference:
And again, to folks who are not vaccinated: You may think you’re putting only yourself at risk, but it’s your choice. Your choice is not just a choice about you; it affects other people. You’re putting other people at risk — your loved ones, your friends, neighbors, strangers you run into. And your choice can be the difference between life or death.
Joe Biden, December 21, 2021See where this is going? “Vaccinate-or-test” will morph into a “vaccinate-or-isolate.” More testing will result in less freedom and more discrimination.
A Better Way. There is another way. If you feel sick, stay home. Find a doctor who will give you early treatment for COVID-19, and test as directed by your doctor. If early treatment doesn’t work, seek higher care at a hospital. When you feel better, go back to your life. Wear a mask for a while if you are concerned about infecting others. These are all commonsense rules taught to us by our parents and used for generations.
Never let test results make you afraid enough to let go of your freedoms.
- What If You Are Wrong?
I am not talking to President Biden, Rochelle Walensky, Anthony Fauci, or anyone else conflicted by political or material entanglements with the pharmaceutical industry. I am not talking to members of VRBPAC or ACIP, or principal investigators for NIH. I am not talking to Bill Gates, Mark Zuckerberg, or anyone who has made billions during the pandemic. I am not talking to anyone who has sold out. If you would do anything to hold onto your research grant, to keep your airline running, or to protect your fiefdom, I am not talking to you. I am not talking to media syndicates with synchronized messages. I am not talking to those cynical about the American dream who think “of the people, by the people, for the people” is naïve and passé twaddle. I am not talking to anyone numb to the pangs of conscience, sociopaths who prioritize greed and power over the lives of others. I am not talking to you because you are already lost. I have nothing to say to you.
I am talking to foot soldiers in the army of the people I am not talking to. I am talking to leaders who have power over people and policies. I am talking to those trying to keep their businesses safe for customers and employees. I am talking to hospital administrators responsible for protecting patients from harm. I am talking to doctors who care about the welfare of their patients. I am talking to elected officials trying to best represent their constituents. I am talking to leaders in the military and law enforcement who protect us from bad people. I am talking to dedicated scientists in public health agencies. I am talking to ethical small business owners. I am talking to HR directors responsible for a healthy and productive workforce. I am talking to all those who want to do the right thing. I know you are out there.
You are leaning on what has worked in the past. You steer a middle course. But as the pandemic evolves, the paradigms have diverged. It is no longer possible to keep one foot on the dock and the other in the boat; the middle ground is now under water. You have chosen the orthodoxy proclaimed by all the people I am not talking to. You feel safer there. Afterall, you are in a delicate situation. You know how things work. You are expected to be a good soldier and toe the line.
I’ve got a question for you. What if you are wrong?

You require vaccines for your employees, you urge boosters for your patients, because aggressive vaccination policies keep the public safe; the unvaccinated are a threat to the health of others. Vaccinate your employees, vaccinate your patients, vaccinate your children. Use the carrot, use the stick, but get it done. But what if universal vaccination will not eradicate the virus? What if the vaccinated can become infected and spread the virus to others? What if indiscriminate vaccination pressures the virus to mutate into more dangerous forms? What if antibody dependent enhancement causes devastating infections in the vaccinated?
You tell others that vaccines are safe and effective. You encourage your patients, your family, your friends to get boosted. Vaccine complications are rare, you say; COVID will shred your lungs, destroy the pleasures of taste and smell, and put you face down on a ventilator. But what if vaccine safety data has been deceptively manipulated? What if you learn of death spikes in populations after vaccines were introduced? What if there is collusion to suppress adverse vaccine safety information? What if the industry reports of vaccine efficacy deliberately leave out measures of absolute risk reduction?
You believe we must protect our children by early vaccination. But what do you do with the evidence that healthy children don’t die of COVID, that vaccination risks for kids far outweigh benefits, and that natural immunity in children is durable?
You say this crisis is no time to question the wisdom of our government’s healthcare policies. Afterall, they’ve been guided by the greatest minds on earth. But how do you feel when you learn that USA has more total per capita COVID-19 deaths than 90% of the nations on earth, and that during the pandemic, average lifespan of Americans has dropped by nearly 2 years, 8.5 times the rest of the developed world? How do you account for the thousands of physicians and scientists who have signed the Global Covid Declaration?
When the FDA tweets, “You are not a horse. You are not a cow. Seriously, y’all. Stop it,” you like it, you share it, but for sure you won’t prescribe Ivermectin or dispense it in your pharmacy. Afterall, there have been no adequately powered, well-designed, well-conducted clinical trials that support the use of Ivermectin in the treatment of COVID-19. You know that treatment for severe COVID is hospitalization, Remdesivir, steroids, and mechanical ventilation. But what if you learn that Remdesivir’s approval was based on inadequately powered, uncontrolled clinical trials that showed shortened hospitalizations instead of improved survival? What if you learned that early treatment keeps people out of the hospital? What if chloroquine prevents infection and spread of SARS viruses? What if the use of approved, off-label, unpatented, repurposed drugs by physicians is really generating the outstanding success rates reported by Front Line COVID-19 Critical Care Alliance, American’s Frontline Doctors, and the Pandemic Health Alliance? What if there has been a deliberate attempt to suppress alternative therapies for COVID-19? What if the leaders of institutions you have trusted for health guidance are manipulating you to enrich themselves and others?
Are you sure that your actions, your decisions, your influence, your mandates are not harming people?
Your decisions affect the welfare, livelihood, and very lives of others. And you are not just deciding for us; you are deciding for our children too. And their children. And all that come after.
Maybe you have been deceived. But what if you are wrong?
- The Booster Trap
First, let’s clear up a misunderstanding. Some people think that a COVID booster is different from a COVID vaccine, but that’s not true. There is no difference between a manufacturer’s booster and its primary vaccine series. Both come from the same vial. There’s been no change in the formulas that were first authorized last year. Pfizer and Janssen boosters are even the dosed the same as a single shot from the primary series. Moderna boosters are half doses of a single shot from its primary series. Either way, the booster shot is just more of the same. If you want to fact-check me on this, read the FDA’s Fact Sheets for the Pfizer Purple, Moderna, and Janssen, the only available vaccines with boosters permitted in the U.S.
There are also those who believe that the vaccines available today are different that the vaccines that were given last winter, but that’s another misunderstanding. The original vaccine was targeted against the Wuhan strain, but even though that strain is no longer present in the community, vaccines given today are the same as the ones first authorized. There has been no change in vaccine formulas. You can fact check me by reading the FDA authorization letters for the available vaccines (Phizer, Moderna, and Janssen) which detail their regulatory histories.
Why the push for boosters? It turns out that the immune response induced by vaccine wanes significantly after 6 months. The booster is thought to drive antibody levels higher, and, the theory goes, it’s the antibody levels that protect the vaccinated from infection. Boosters have been authorized for all Americans over 18 years of age, 6 months after completion of an mRNA primary vaccine series (Pfizer and Moderna) or 2 months after the Janssen injection. Janssen’s booster interval is shorter because Janssen has the lowest immunogenic effect of the three authorized vaccines. Janssen-induced antibodies wane earlier.
Everything above this paragraph is an objective report of the current vaccine landscape. Now I’m going to predict the future. When I look in my crystal ball, here’s what I see coming.
Janssen will go from a single injection to a two-shot series, separated by 6-8 weeks. Then Janssen’s booster interval will be set at 6 months, just like the other vaccines. So far, only one booster has been authorized, but expect booster authorizations to go on an every six-month renewal cycle.
The definition of “fully vaccinated” will change to include a current booster. If it’s been more than six months since your last booster, your vaccination status will expire. It will take a computer to keep up with everyone’s expirations, so vaccine passports will be tracked on your smartphone. This passport will be connected to other data on your phone—where you go, what you tweet, who your friends are—to create a social credit score that will be used, along with your vaccine passport, to restrict or permit access to products, services, and transportation. Since your financial institutions are probably already connected to your smartphone, it will only take the flip of a switch to turn off access to buying power. That should incentivize citizens to maintain good scores.
And what about those boosters—will they ever change? Probably. The mRNA technology used in Pfizer and Moderna vaccines is a platform that can be adjusted rapidly to changing vaccination targets. As the virus mutates, these vaccines can be quickly reengineered to respond to the changes, perhaps even without additional FDA submissions. And it will be used for more than SARS-CoV-2. Other vaccine targets can be loaded on the platform to create a vaccination cocktail tailored to the pandemic du jour. And it will be used for more than vaccines. Other gene therapies can be mixed into the brew, all for your safety of course. You’ll be a much happier, more compliant, and easily manipulated citizen. The possibilities are endless.
What do you think of my crystal ball? Personally, I don’t like it very much. It’s not a world where I want to live. If my predictions become true, we lose the freedom to make personal choices. Free will, the essence of humanity, will be gone. That’s not for me.
We still have a choice. We can choose to go down this road of boosters without knowing where the road will lead, or we can recognize that vaccination will not eradicate this virus, no matter how many boosters we take. If boosters will not eradicate SARS-CoV-2, there must be another reason to inject the world with limitless mRNA sequences.
I don’t want to find out what that reason is, so I’m not going down that road. My humanity is too valuable to me.
- The Omicron Variant
A new variant is sweeping the globe. Today, the WHO designated the b.1.1.529 variant a Variant of Concern and assigned it the name Omicron, humorlessly passing on the opportunity call the new variant Nu. The Omicron variant, first identified earlier this month in South Africa, has already spread to Israel, Hong Kong, and Belgium, prompting travel restrictions by many countries.
There’s much more to learn about this variant, but reports so far suggest this is a highly mutated form with cluster mutations in the receptor binding domain, the portion of the spike protein where vaccine immunity is aimed. It’s reasonable to infer that these mutations may lead to increased vaccine escape. More breakthrough infections can be expected.
According to an article published in Nature yesterday, there are already anecdotal reports of reinfections and cases in vaccinated individuals. If the infectivity of Omicron is as least as high as Delta, expect Omicron to soon replace Delta as the dominant form in the U.S.
As the virus continues to evolve, the vaccines remain static. The vaccines available today were designed to provide immunity against the spike protein of the wild type strain identified in Wuhan in January 2020, but that viral strain has practically vanished. As the virus continues to move, individuals who are only protected by vaccination will be increasingly exposed to virus attacks.
Those who have been previously exposed to the virus can be expected to have broad immunity. Think of castle walls deflecting missiles launched from many directions and angles. Those protected by vaccine alone have neutralizing antibodies against the wild-type spike protein. Think of the protection provided by a slender pole. An attacker needs only move over a few feet to obtain a direct line of sight to the target. That’s why breakthrough infections are common, why vaccinated individuals can transmit the virus, why vaccinated individuals require hospitalization, and why vaccinated individuals die from COVID-19.
One more point about variants. The CDC now has four variant classes, listed from least to most significant: Variant Being Monitored (VBM), Variant of Interest (VOI), Variant of Concern (VOC), and Variant of High Consequence (VOHC). In April 2020 there were many variants on the VOI and VOC lists. However, as vaccination rates increased, all but one of these variants disappeared from the United States and were moved to the VBM list, including the Alpha variant responsible for the COVID-19 spike last winter. The Delta variant and its rare sublineages are the only remaining Variants of Concern.
As the virus continues to evolve, a variety of variants should be expected, but instead we find a monotypic variant population. This suggests unnatural manipulation, and this observation is coincidental with the continued push for vaccination by a first-generation vaccine. Could there be a causal relationship? Could the Omicron variant be a result of the vaccination policy advocated by national and international health organizations? We don’t know for sure, but it is plausible. What we do know is that this virus will be with us for some time. Universal vaccination will not eradicate SARS-CoV-2. We must look elsewhere if we are going to live with the virus.
Early treatment shows the most promise.
- Boosters for All
Yesterday, the FDA revised the Factsheets for Providers Administering Pfizer BioNTech (both Purple and Gray) and Moderna COVID-19 Vaccines, permitting boosters of these unapproved products to Americans 18 years of age and older because of an ongoing emergency. The FDA took this action without reconvening the Vaccines and Related Biological Products Advisory Committee, a panel of national health authorities.
Yesterday’s action overrules the recommendation made by the Advisory Committee at its 167th meeting on September 17 when the panel voted 16-2 against the question, “Do the safety and effectiveness data from clinical trial C4591001 support approval of a COMIRNATY booster dose administered at least 6 months after completion of the primary series for use in individuals 16 years of age and older?” True, the previous question was for 16 and above, not 18 and above, but the spirit of the committee discussion was for targeted boosters, not blanket boosters.
According to the FDA press release issued yesterday, “The FDA did not hold a meeting of the Vaccines and Related Biological Products Advisory Committee on these actions as the agency previously convened the committee for extensive discussions regarding the use of booster doses of COVID-19 vaccines and, after review of both Pfizer’s and Moderna’s EUA requests, the FDA concluded that the requests do not raise questions that would benefit from additional discussion by committee members.”
This action comes days after Alex Berenson, formerly of the New York Times, reported an error in Pfizer’s publicly reported safety data. Initially, Pfizer reported that two vaccine recipients died during trials, compared to four placebo recipients. In a July update, the count was revised to 21 deaths among vaccine recipients compared to only 17 in placebo recipients.
Then there’s FDA’s response to a freedom of information act (FOIA) request on Pfizer’s COVID-19 vaccine. Instead of transparency, the agency filed a petition in U.S. District Court to delay its response for 55 years.

Vaccine chart, updated for new EUAs issued on November 19, 2021. Up to now, I’ve just been reporting the news, but here comes commentary. These facts create a disturbing trend. What could they be hiding? I’m forced to one conclusion. The FDA and the pharmaceutical industry are colluding to coverup data and debate so they can sell vaccines. If you can reach another conclusion rationally, please tell me. I can’t.
The events of last week occurred in the open. Imagine what’s happening out of view.
- Censored
My most recent blog about vaccines for children was removed by LinkedIn because of a violation of LinkedIn’s Professional Community Policies. Although LinkedIn won’t tell me what specifically provoked removal of my article, I must have somehow run afoul of this sentence in their policy, “Do not share content that directly contradicts guidance from leading global health organizations and public health authorities.”
It’s not just LinkedIn. Twitter has a lengthy policy on COVID-19 tweets, including a ban on misleading information about “the safety or efficacy of treatments or preventative measures that are not approved by health authorities.” Referring again to “government health authorities,” Facebook’s policy explicitly lists examples of prohibited claims about vaccine effects such as “Bell’s palsy,” “blood clots,” “death,” or the emergence of a “new COVID-19 [sic] strain” with such authority that it would be an exquisite piece of satire if Facebook were not so sadly unaware of its naivety. I stopped looking for more examples of Big Tech’s holier-than-thou-know-it-all-ism quite confident that I could find as many as I wished.
The question is inescapable. When “health authorities” disagree, how does Big Tech decide which position is right and permissible, and which position is wrong and censorable? When an observation contradicts its orthodox viewpoint, Social Media labels it false and removes it. According to Thomas Kuhn in The Structure of Scientific Revolutions, unorthodox observations should be highlighted since they power the movement of scientific understanding.
But let’s not get into the science. Let’s talk about disagreements among government health authorities. About the same time that USFDA permitted Pfizer-BioNTech COVID-19 Vaccine for emergency use in children 5 to 11 years old, Taiwan halted plans for vaccinating those less than 12 years old, France’s Haute Autorité de Santé advised against Moderna vaccination for anyone less than 30 years old, Finland prohibited the vaccine in the same age group, and Denmark and Sweden prohibited its use in anyone under 18 years old. While other countries are restricting the use of mRNA vaccines in young people, USA is vaccinating preschoolers.
Outside government sponsored health organizations there is also disagreement about safety of vaccines in young people. Although 17 members of the Vaccines and Related Biological Products Advisory Committee voted that the benefits of vaccinating children aged 5 to 11 outweigh the risks, the opposite opinion is held by over 13,000 international physicians and scientists who have signed the Global Covid Summit Declaration II.
It’s clear there is a lack of consensus among “leading global health organizations” and “public health authorities.” Yet U.S. government officials are using intimidation, ridicule, and disregard for legal process to make it appear the issues driving its public health policy are settled. It’s just not true.
A vigorous public debate is needed, and social media could facilitate it. But social media is not content to be the platform for debate. Instead, it wants to control the outcome. Without years of deliberate study and armed only with a crash course in medical science, social media proclaims itself the ultimate health authority, deciding what observations are fit for public consideration and hiding the rest. Abandoning its journalistic legacy as the fourth estate, social media has become the stooge of government. Because the first amendment prevents it from doing so directly, the government is using social media as its proxy to restrict the speech of Americans.
It’s not funny. It’s no longer just our lives; the lives of our children are at stake. Just as physicians have a duty to “do no harm,” parents have a duty to prevent harm to their children. Quoting the best social media post I saw last week, “Don’t let your children die on the hill you refuse to fight on.”
- Color Coded Vaccines
On October 29, the FDA removed the combined COMIRNATY/Pfizer-BioNTech Fact Sheet for Healthcare Providers. In its place, the FDA issued three new Fact Sheets for Healthcare Providers Administering Pfizer-BioNTech vaccines, one for each of the now three versions of the product which are distinguished by vial cap colors. Vaccine vials with purple caps are authorized for individuals 12 years of age and older and must be diluted before injection. Vaccine vials with orange caps are authorized for children 5-11 years of age and must be diluted before injected. Vaccine vials with gray caps are authorized for undiluted administration to individuals 12 years of age and older but are not available in the United States.
Sound complicated? It is. And it raises disturbing questions. But first, here’s an updated (and complicated) vaccine chart:

Now the questions.
Is there an FDA approved vaccine for children under 16 years of age?
No. COMIRNATY is FDA approved for individuals 16 years of age and older. Quoting from the Pfizer-BioNTech Orange Fact Sheet, “The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) to permit the emergency use of the unapproved product, Pfizer-BioNTech COVID-19 Vaccine, for active immunization to prevent COVID-19 in individuals 5 years of age and older.”
Why did the FDA approve COMIRNATY if it’s not available in the United States?
I don’t know for sure, but I can speculate. The FDA News Release on August 23 makes it seem as if Pfizer-BioNTech is an approved vaccine. This may be the reason for COMIRNATY’s approval—to provide a veneer of legitimacy to the authorizations for boosters and child vaccines that followed. The Fact Sheets are clear: Pfizer-BioNTech vaccines are not approved. Not for anyone.
Why is COMIRNATY not yet available?
In the emergency use authorization letter for Pfizer-BioNTech reissued on August 23, the FDA acknowledged that, “There remains, however, a significant amount of Pfizer-BioNTech COVID-19 vaccine that was manufactured and labeled in accordance with this emergency use authorization. This authorization thus remains in place with respect to that product for the previously-authorized indication and uses.” In other words, FDA will allow Pfizer’s inventory to be consumed under EUA before requiring production and distribution of COMIRNATY. By the way, you’ll have to go to web.archive.org to find this letter. I can no longer find it on FDA’s active website.
If COMIRNATY is not yet available because of Pfizer’s vaccine inventory, how does Pfizer manufacture two new versions (Gray and Orange) of its vaccine so quickly?
Good question. Is Pfizer just consuming inventory or is Pfizer producing new vaccine? I don’t know for sure, but it seems to me Pfizer is producing new vaccine.
Why did the FDA authorize Pfizer-BioNTech Gray if it’s not available in the United States?
I’m puzzled by this question. How can the FDA authorize use of an unapproved product for an emergency when that product is not available? If you have an idea, please tell me.
Are all COVID Vaccines experimental?
Yes. There is not an approved, licensed COVID vaccine available in the United States. All available vaccines are unapproved products permitted for emergency use only. It’s a big experiment. Vaccinated individuals are part of the experimental group. Unvaccinated individuals are part of the control group. We will analyze the results in a few years.
Can I or my child be forced to accept a COVID Vaccine?
No and Yes. Fact Sheets for Healthcare Workers Administering Vaccines say that the person administering the vaccine must disclose that “the recipient or their caregiver has the option to accept or refuse” the COVID-19 Vaccine. Fair enough, but this hasn’t prohibited vaccination by coercion. There are many people who have been forced to accept a COVID vaccine to keep their jobs, and people who refused vaccination have lost freedoms and employment. Coerced consent is and always will be unethical.
Are we sure Pfizer-BioNTech Orange COVID vaccines are safe for children?
No, and this is the most disturbing part of the October 29 actions. The CDC insists the vaccines are safe for children. But many prominent physicians have disputed this claim, saying that long term effects of vaccines on children are unknown. I agree. Without a time-machine, it’s impossible to know the future effects of vaccines given to children today. But I’m not the only one who thinks this way. At the 170th meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee, Dr. Eric Ruben, Editor-in-Chief of the New England Journal of Medicine and temporary voting member of the committee, said, “We’re never going to learn about how safe this vaccine is unless we start giving it. That’s just the way it goes.” Dr. Ruben voted for authorization of experimental vaccines in children. Whatever you think of his judgement, at least he’s honest about the safety data. We don’t have any yet.
- Break Free
The real division is not between conservatives and revolutionaries
but between authoritarians and libertarians
–George Orwell, 1948
The President is losing patience. Six quarters into the emergency, the FDA has authorized COVID-19 vaccines down to five years of age. The CDC maintains these vaccines are safe and effective. Vaccinations are mandated by powerful employers, high ranking generals, and top government officials. Most of the medical community are on board. Failure to comply costs income and freedom. It’s intimidating. Many have submitted to the pressure. These policies have concentrated authority and power in a few “experts” who presume to know what’s best for everyone else. It’s not just arrogance. It’s slavery.
Slavery doesn’t need a plantation and rows of cotton. Slavery occurs when one person owns the thoughts and actions of another. Motives don’t matter. Good intentions don’t justify coercion. Masters who treat their slaves well are still slaveowners. The core moral flaw of slavery is the notion that one person can own another. Slaves exist to serve masters, not the other way around.
Masters cannot make decisions in the best interest of their slaves. The interests of the slaveowner always have precedence. If you own my decisions, you own me. You can’t make the best decisions for me because you don’t know what’s important to me. The individual taking the risk must have decisive control. Today’s public health policies transfer choice from individuals to powerful experts just like slaves surrender control to their masters.
We don’t need experts to understand the issues of the pandemic. COVID-19 is bad. Many people have died, more than should have. But we’ve learned to identify those at risk. Sound, compassionate public health policy would focus attention on the vulnerable and protect them with more than vaccines. Instead, our masters are using only one tool and applying it universally.
Vaccines have risks. Many people have died, more than should have. Vaccines were rushed to market with only a thin veneer of study and testing. What we know of vaccine risks—myocarditis, blood clots, neuromuscular disorders, death—is scary enough. What we don’t know is even scarier. Some of these potential future problems can be deduced from the studies requested by the FDA in its COMIRNATY approval letter.
Yet our experts cling to a universal vaccination policy that seems to be less in the public interest than in that of vaccine vendors. Our impatient masters have cornered us into a company store where there’s only one shoddy product for sale. We must break free.
America is founded on liberty. Yes, our history is filled with cognitive dissonance on this point. The institution of slavery is baked into our founding documents, right alongside guarantees of individual rights and freedoms. But the understanding of liberty is also baked into Americans, so much so that we were willing to shed blood to purge slavery from our land, without the assurance that we could.
We’ve reached a similar moment. Echoing notes from the Gettysburg Address, history has given us the opportunity to purge a more occult and subversive form of slavery from our land. Our public health policies have devolved to the coercion by the few over the lives of the many. These policies have shifted from information to dogma, from recommendations to requirements. Like the slaves of old, we must adopt the religion of our masters and submit to their commands. Otherwise, we are promised discomfort.
To those subjected to these policies, my message is simple. Resist this coercion like it’s slavery. It is.
- Vaccine Booster Update
The FDA reshaped the vaccine landscape last week, authorizing single boosters for Moderna and Janssen vaccines, and permitting boosters from all vaccine manufacturers regardless of the initial vaccine brand. Here is an updated vaccine chart, incorporating these changes.

The changes were discussed at the two-day Advisory Committee Meeting on Vaccines and Related Biological Products Advisory Committee, held October 14-15, 2021. EUA applications for single boosters of Moderna and Janssen vaccines were unanimously recommended (4:26:25). The committee heard a report on the NIH “Mix and Match” study (5:27:26), the basis for the booster interchangeability authorization, but did not vote. After this meeting, FDA approved booster interchangeability and updated Fact Sheets for Healthcare Providers Administering Pfizer, Moderna, and Janssen vaccines. These Fact Sheets still say there is “no information on the co-administration” of vaccines. The rules for interchangeability between primary and booster vaccines are based on the vaccine used for the primary series. By these rules, anyone over 18 years old can get a Moderna or Pfizer booster 2 months after an initial Janseen injection.
FDA Approval means that a drug, treatment, or medical device has been licensed by the FDA for a particular purpose. Contrary to what you may hear, approval is not a guarantee of safety and efficacy. Rather, it means that the item in question has been through FDA’s rigorous gauntlet designed to prevent worthless or harmful products coming to market in the United States. Approval is different from authorization. FDA Authorization means that a product is available by Emergency Use Authorization, also known as EUA. The EUA process is designed to speed availability of products in the U.S. during an emergency. “Off Label” is a term used to describe use of an approved drug or device for a purpose other than its express licensed intent. Off label use of drugs is common practice. “Not authorized” is a term used to describe use of a drug or device which has neither been approved by the FDA nor made available by EUA.
Two key criteria for EUA are that an emergency exists, and there are no approved products to address the needs of the emergency. The continued availability of COVID vaccines under EUA is problematic on both points. First, as COVID-19 returns to endemic levels in many parts of the country, it’s debatable whether an emergency still exists. Once an emergency passes, and all EUAs, including the authorizations for vaccines, should be withdrawn. Second, there is an approved COVID vaccine: COMIRNATY. By approving a product that is not available in the U.S., the FDA has twisted itself into a pretzel. If the product is unavailable, it should not be approved. If the product is approved, EUAs for the other vaccines should be withdrawn. The FDA changes its call from heads to tails depending on how you flip the coin.
Expect two additional significant changes in coming weeks. The first will be the push to vaccinate children. The second will be the definition of “fully vaccinated” to include boosters. This will be followed by authorization for multiple boosters, meaning that you will always be just months away from losing your “fully vaccinated” status. Vaccine passports will then be a reality in the United States. Maybe that was the endgame all along.
Who would have thought this is where we would be 21 months ago?
- Belief and Knowledge
I am not a scientist, but I love science. I am not a theologian, but I love theology and the effects of spirituality on my life. Just like I am a practitioner of pathology, I am also a practitioner of faith. I am enriched by both.
Religion deals with matters of belief. Science deals with matters of knowledge. Both address the big questions of life—”Why are we here?” “Where are we going?”—but from different perspectives. One is not a backstop to the other. Beliefs are not morally inferior to knowledge, just as knowledge is not morally inferior to beliefs. Both are important, but they live in different realms. Innocently confusing science and religion leads to superstition, ignorance, or harmful conclusions. Deliberately confusing science and religion is a deception that robs us of material and spiritual treasures.
Falsification is a key distinction between belief and knowledge. A scientific claim is falsifiable, meaning it must make a prediction that can be tested by experiment. If experimental results are not what the claim predicts, then the claim is false. But if experimentation supports the claim, it’s not necessarily true; it simply might be true. The scientific process is a last man standing game. The longer a claim stands, the more likely it is to be true. At some point, when an idea becomes more likely than anything else, we call it knowledge. But knowledge is, and always has been, what is most likely true, not what is certainly true. We can only have scientific certainty about what is false.
Lack of certainty isn’t the only limitation of knowledge. There are scientific horizons, and we cannot see what’s on the other side. For example, the universe is most likely expanding, but expanding into what? We cannot know. If the universe is expanding, then it must have been smaller before, and even smaller before that, and so on until it’s a tiny universe holding all matter and energy. But what happened before that? We cannot know. What’s outside the event horizon of light, or the gravitational horizon of black holes? Does our physics work there? Can alternate universes coexist? We can hold beliefs about these things, but these questions are not in the realm of science. We have no applicable knowledge because we have no power to observe.
Science has significant limitations. We can never be certain about what science tells us, and there are some questions that are not open for scientific investigation. Religion also has limitations, but different ones. Religious claims do not have the requirement of falsification. Omnipotence is the ultimate answer for all religious questions. When there’s no experiment that can demonstrate an idea to be false, it cannot be science, but it can be religion. Science requires falsification; religion requires faith. Faith and beliefs are good things. They give us hope, purpose, and compassion. Science cannot.
Despite its limitations, science is a powerful tool that augments our understanding of reality. We cannot rely on science to give us quick answers, so during this pandemic, we must have faith—lots of faith. But we also must speed science along by testing as many ideas as possible, all at the same time. A pandemic response that clings to ideas which are demonstrably false and dismisses competing ideas without experiment is not based on science. It’s religion pretending to be science, and it’s dangerous. There are three explanations for nonsense disguised as science: foolishness, greed, and evil. I fear that all three are now hopelessly entangled.
Religion and science have important roles in our fight against the pandemic. Understanding the difference between them is a protection against deception. When someone says, “believe in science,” beware of fraud. Your life, your liberty, and your sacred treasures are at risk.
- Stop Calling It Science
Medicine is my professional life. Science is the language of medicine, or at least it used to be. I’m not a scientist; I’m a practitioner. But I love science, just like I love ideas. Ideas separate humans from other living organisms, and ideas are often played out in the arena of politics. I am not opposed to politics, but I am opposed to deception. It is deceptive to hide behind the label of science to cover political actions.
I don’t believe today’s misuse of science is accidental. Those doing it are too smart and too well educated to make that mistake. Phrases like “follow the science” and “scientific close call” give an air of legitimacy to policies that are driven by agenda rather than facts and knowledge. Counter examples are ignored; theories are not allowed to be disproven.
Today’s orthodoxy is defined by elite high priests who possess secret gnostic knowledge. Scripture is what the priests say it is. Ordinary people have no access their secret data. Opponents of orthodoxy are labeled heretics, and some are vilified as examples to those tempted to stray. There are rites that involve the letting of blood, and these rituals must be repeated periodically to maintain continued salvation. Mass demonstrations of faith by believers prove their devotion to a movement that promises a second coming of pre-pandemic life sometime in the distant future, even though exactly when and how that will happen is vague. Occasionally, human sacrifice is required to appease the gods, but those chosen for sacrifice must not complain. The lambs must accept their fates willingly. There can be no dissent. Heterodoxy is not permitted in a nation whose motto is “In Science We Trust.”
This is not science; this is religion. Despite the first amendment to our constitution, our country is being turned into a theocracy, worshiping at the altar of “scientism.” Scientism is being used as a tool to advance a political agenda, not a scientific one.
Science is a process that establishes our best understanding of truth by disproving all that is false. Someone says, “I have an idea,” and other scientists set out to prove it false by experiment. “If your idea is true,” the experimenters say, “then my experiment should work out this way; since it worked out that way instead, your idea must be false.” Experiments never prove an idea true. “Scientific truth” is a probability not a certainty. It’s subject to revision when someone invents a better idea, shifting our understanding into a new paradigm.
Skepticism is integral to the scientific process. When doubt is not allowed, it may be many things, but it’s not science.
- Winning the War Against Therapeutic Nihilism
Dr. Peter McCullough spoke to the Association of American Physicians and Surgeons at their annual meeting on Saturday, October 2. He gives a clear, easy to follow, scholarly perspective on the causes and treatments of COVID-19 and the safety and efficacy of COVID vaccines. It’s a little more than an hour long, but I recommend you stop reading this blog and watch it by clicking here. If you don’t have an hour to watch the video right now, here are my CliffsNotes version of Dr. McCullough’s talk, complete with video references.
There are serious safety concerns with COVID vaccines. Lapses in usual safety standards plagued vaccine development and distribution (8:10). Groups excluded from pre-authorization clinical trials are receiving vaccine (9:13), including pregnant women, women of childbearing age, COVID survivors, people with suspected COVID, and those with positive COVID serologies.
The CDC and FDA have misled the public about vaccine safety. They minimized vaccine related deaths (14:14), and they have not provided periodic safety reports. Despite what is reported in the media, the FDA did not approve Pfizer-BioNTech COVID-19 Vaccine (22:10). The CDC manipulated data to support the “Pandemic of the Unvaccinated” narrative (29:15). Of Americans hospitalized patients with COVID during the delta wave, 23% have been vaccinated (32:20). The CDC and FDA have failed to emphasize that seniors suffer the most vaccine failures (30:20). Instead, they are focused on authorizing vaccines for children, a group that has a greater risk of hospitalization for vaccine-induced myocarditis than for COVID-19 (18:16). The CDC and FDA cannot be trusted to provide honest information about vaccines.
The universal vaccination policy must change. All vaccines have failed against the delta variant (26:45), and they have not stopped the spread of virus (23:57). Vaccines are forcing viral mutations (34:05); as vaccination rates increase, natural viral diversity decreases. Vaccines produce narrow, limited immunity (36:00), and vaccinating COVID survivors causes harm (49:19). Vaccinated individuals are as likely to spread virus as unvaccinated individuals (37:07). On the other hand, natural immunity is robust, complete, and durable (49:09). Natural immunity is the only backstop to virus spread (50:00).
Treatments, not vaccines, drive down COVID mortality (33:43). COVID-19 is a complex disease, but early home therapy is effective (38:30). Inadequate treatment is responsible for COVID-19 deaths (44:34). Many seniors have been abandoned by their doctors (45:47), but A Guide to Home Treatment of COVID-19, made available free by the AAPS, fills gaps in management (46:39).
People are losing human rights. Basic freedoms are now dependent on vaccine status (50:24). We need outrage over ineffective and unsafe vaccines (52:45), we need doctors to be doctors (54:35), and we need journalists who recognize that something is wrong (56:36), that there has been a suppression of treatment resulting in fear, suffering, loneliness, isolation, hospitalization, and death (56:50).
But my notes do not have the eloquence and power of Dr. McCullough’s own words. Please, click here and listen to five minutes, then stop when you want. If you can.
- A Physician’s Descent into the Abyss
Next to my wife and family, medicine is my life. I go to work in a hospital almost every day, and while I’m there, I’m focused on the patients whose blood, fluids or tissues come to my attention. I give them the very best I can, not perfectly, but humanly. Many patients aren’t aware that pathologists exist, but if you’ve ever been on a Hero’s Journey involving cancer, you know who I am. I was there at your jumping off point. I’m the one who signed your biopsy report, giving you the information needed to face the monsters of your quest. I’ve never personally experienced cancer, although both my wife and I have fathers who did, but I see cancer up close daily, and I frequently encounter those on the cancer journey.
Here’s a short summary of the Hero’s Journey. A hero candidate is called out of ordinary, mundane life to go on a quest. The candidate initially resists but is eventually drawn to the edge of the abyss and outfitted for the journey. Descending into the darkness, the hero enters a fantastic, dream-like world where rules of ordinary life don’t apply. Think Star Wars, Alice in Wonderland, or Odysseus in Hades. Real dangers are encountered, and sadly, not all heroes survive. But those that do come back to the ordinary world changed, and they share their wisdom with the generations. Joseph Campbell’s masterful articulations of the Hero’s Journey demonstrate that this formula transcends cultures and epochs. Cancer survivors know what I’m talking about because they’ve been on a Hero’s Journey.
Although I don’t feel much like a hero, COVID has sent me tumbling out of my ordinary world into an abyss. My pre-pandemic world was based on trust. Physicians are taught to think for themselves, but to doubt themselves at the same time. More than anything else, our education and training teach us that we just don’t know enough. There’s always someone smarter or intellectually more energetic, someone who dives deeper or stretches broader than we can ever hope to do. Yet there’s something about this humiliating self-awareness that gives us the tools we need to help those in the ordinary world with their ordinary health problems. We frequently consult trusted references, colleagues, and experts, and as we do, it slowly begins to make sense. Experience gives us confidence, and that confidence is transferred to our patients. Physicians become the handles patients hold onto when the earth drops beneath their lives.
The pandemic has changed all that. Physicians feel compelled to take sides. You either stand with most of your colleagues and friends, medical associations, and trusted institutions like the FDA and CDC, or you stand with what has made sense to you throughout your career. The pandemic has made this an either-or proposition. Like 1984, it’s a battle between your thoughts and the thought police; you either participate in the Two Minutes Hate enthusiastically, or you risk vaporization.
My trust in the CDC began to wane in May when, in contradiction to my education and training, the agency insisted on vaccination of COVID survivors. My trust was further depleted when I realized testing would not be used to guide vaccination decisions despite years of established pre-pandemic practice. Now, there is contradictory information published on CDC and FDA websites, and disregard for approval and authorization processes. Yet even the act of pointing out these discrepancies separates you from the herd like a calf in a cutting horse competition.
I have decided to stand for truth with the confidence instilled by my education, training, and experience, no matter what. There’s a lot in that “no matter what”—isolation, ridicule, coercion. But if you don’t have your thoughts, you don’t have your humanity. Humans are not required to believe alike, but they are required to believe. I am determined to crawl out of the abyss, humanity intact, back into the ordinary world, dragging as much trust with me as I can carry.
Maybe some of my colleagues will identify with what I’m saying.
- Deception
Misconceptions about COVID Vaccines are fueling vaccine mandates. The CDC has contributed to these misconceptions by its recent statements and actions. Trusted institutions and processes are now corrupted by a political agenda that has licensed vaccine mandates. Next will be vaccine passports and social credit scores, resulting in the loss of human rights.
Last week, FDA published a new combined Vaccine Information Fact Sheet for Recipients and Caregivers About COMIRNATY (COVID-19 Vaccine, mRNA) and Pfizer-BioNTech COVID-19 Vaccine to Prevent Coronavirus disease 2019 (COVID-19). This Fact Sheet explains the distinction between Pfizer-BioNTech COVID-19 vaccine and COMIRNATY (COVID-19 Vaccine, mRNA). This document states that the two vaccines “can be used interchangeably,” but are “legally distinct” (see footnote 1). COMIRNATY (COVID-19 Vaccine, mRNA) is an FDA-licensed vaccine for individuals 16 years old and older; Pfizer-BioNTech COVID-19 Vaccine is an authorized vaccine for individuals 12 years and older. COMIRNATY inherits Pfizer-BioNTech’s EUAs; Pfizer-BioNTech is not grandfathered into CORMINATY’s license.
The new Fact Sheet also expands emergency use authorization for third shots (boosters) of both vaccines. In doing so, the FDA followed the spirit, if not the letter, of its independent Advisory Committee Meeting on Vaccines and Related Biological Products Advisory Committee September 17, 2021 (watch following 7:42:00).
On the other hand, the CDC’s information and guidance has been confusing and misleading. On its website, the CDC ignores the legal distinction between the two vaccines so carefully parsed by the FDA, inaccurately lumping them under the label “Pfizer-BioNTech (COMIRNATY) COVID-19 Vaccine” and saying that the FDA approved this vaccine on August 23. That’s not exactly true. But the misinformation has taken root. Even factcheckers are spreading the false claim that Pfizer-BioNTech and COMIRNATY vaccines are legally equivalent.
Last week the CDC went further, recommending boosters for individuals not included in the FDA’s Emergency Use Authorization in contradiction to the CDC’s own Advisory Committee on Immunization Practices. Dr. Rochelle Walensky, director of CDC, justified this action (watch following 27:57) by saying it was a “scientific close call,” (28:22) and that she would have voted in favor of the recommendations if she were part of the committee (28:36). But she wasn’t part of the committee, and it wasn’t a close call.
Close calls are judgments made on the sports field, risk calculations during a game of chess, or complicated ethical determinations. Close calls are decisions made with incomplete information, under the stress of time, that exceed our computation ability. None of this describes science. Science is a method that either disproves an idea or does not. There are no “scientific close calls.”
The CDC overstepped its jurisdiction. The FDA, not the CDC, issues emergency use authorizations. Yet now CDC guidance is at odds with FDA’s EUA, bypassing the safety afforded by this carefully thought-out process.
There was a reluctance to embrace vaccine mandates until FDA licensed a vaccine. On August 23, the FDA licensed a vaccine which is still not available. Instead of giving us a licensed vaccine, the FDA gave us a license to mandate vaccines. In August, the White House promised booster shots by September 20. Last week boosters were made available under CDC guidance via a short-circuited process. This is not science. This is politics.
These are smart people who have studied logic and rhetoric at the finest colleges and universities in the land. They should know better. They do know better. This is deliberate and bold deception. Trusted instructions of science and medicine have been corrupted to further a political agenda. Now that we’re out of the realm of science and in the world of politics, speculation runs wild. My speculation is that someone wants to sell vaccines, and lots of them. My speculation is that vaccine mandates will lead to vaccine passports and social credit scores which will eliminate our human rights. No wonder there’s a crisis of trust in America.
- Long COVID
COVID-19, the disease of the pandemic, has two pathways. In one pathway, viral infection directly causes the upper respiratory symptoms like runny nose, cough, fever, sore throat, and, in severe cases, pneumonia and respiratory failure. The second pathways is associated with some of the more confounding symptoms of COVID-19 like loss of taste and smell, myocarditis, pericarditis, cardiac arrhythmias, migraines, cognitive deficits, Guillain–Barré syndrome, Bell’s Palsy, and blood clots. These symptoms sometimes appear with infection, but often they emerge after the acute illness is over, and they may last a long time. This is what is known as “Long COVID.”
Long COVID doesn’t happen to everyone infected by the virus. It seems to affect women more than men, and the middle-aged more than the very young or the very old. But for those affected, long COVID can be painful and debilitating.
There are several ideas about what causes Long COVID. One plausible idea is that the immune response mounted to fight SARS-CoV-2 attacks the body’s own cells. In other words, Long COVID may be an autoimmune disease. Viewing this phase of COVID-19 as an autoimmune disease forms the basis for the use of drugs known to tamp down the immune response as an early treatment or preventative for COVID-19. These drugs may also help patients who are struggling with long COVID symptoms.
It’s intriguing that many vaccine complications overlap with long COVID symptoms. Vaccine fact sheets contain warnings for myocarditis/pericarditis, blood clots, and Guillain-Barré Syndrome. These are all immune-mediate processes—in other words, autoimmune disease from an immune system primed to attack your own body. Vaccination is designed to mount an immune response to the spike protein, the tool the virus uses to pick the lock on the door to your body. If Long COVID is an autoimmune response, it’s not surprising that vaccination may cause a similar response.
Another intriguing observation made by me and some of my colleagues, but one I’ve not found published, has to do with the timing of adverse effects of vaccination. I want to be clear that adverse effects of vaccination seem to be rare. Yet, complications occur. The observation is that people who’ve had COVID-19 before taking a vaccine seem to have adverse effects of vaccine immediately if they have them at all. Alternatively, people who have never had COVID-19 have adverse effects of vaccine weeks after vaccination if they have them at all. It makes sense that people who’ve had COVID-19 have an immune system primed for an immediate response, while those that have never been infected need time before the effects are seen.
These observations bring up a couple of questions. Can vaccination cause an autoimmune disease like Long COVID? And if so, will treatments for Long COVID be helpful to those people?
There’s still so much we don’t know.
- COVID Serology
The immune system is a big complex machine. Medicine tries to simplify the machine to make it understandable and to manipulate it to our advantage. That’s why we measure antibody levels in the blood. The measurement of antibody levels in the blood is called serology. Serology doesn’t measure the whole immune system, but we do it because it’s easy, and it gives us an idea of what’s going on.
Your immune system is stimulated by molecular structures that are not native to you. You could say that your immune system is xenophobic, reacting against foreigners. And your immune system has a long memory. Once stimulated, these memories allow your immune system to mount a defense quickly should that foreigner ever be encountered again. For many infectious agents, including SARS-CoV-2, this means the formation of antibodies which can be measured in your blood.
When you are infected by the virus, your immune system is exposed to all the molecules that make up that virus. Your immune system can respond to any of those molecules, including one special molecule: the spike protein. We need to understand what makes spike protein so special.
Contact between the spike protein on the SARS-CoV-2 virus and a cell inside the nose is the first step in the infection of our bodies by these tiny invaders. The spike protein is like a key that unlocks the vault, giving the virus access the interior of the cell. Once inside, the virus hijacks the cell machinery, converting it into a virus manufacturing plant. Thousands of copies of the virus are pumped out which infect neighboring cells, and the process repeats.
Antibodies to spike protein are special because they are neutralizing antibodies. Neutralizing antibodies get between the viral key and the cellular portals, acting like putty gumming up the keyholes. That’s why code for spike protein is the active ingredient in mRNA vaccines, and that’s why we should be able to measure vaccine response with spike protein antibodies. Other parts of the immune system are activated too, but these work after the virus has entered the body. At least that’s the theory.
How well does all this work? Imperfectly.
While vaccination may reduce the risk of future infection, it does not prevent it. Breakthrough infections occur. Maybe that’s because neutralization only happens when antibody levels are high enough. Or maybe neutralizing antibody levels fade within months of vaccination. Or maybe the small alterations in spike proteins of variants make vaccine-induced neutralizing antibodies less effective. Or maybe it’s a combination of all these ideas. We really don’t know.
And there’s the point. We really don’t know. We certainly don’t know enough to make universal vaccination the sole objective of our pandemic response. Vaccination is a tool that can be used to keep people alive, but it should not become the primary goal. Other theories need to be investigated to identify our best hope for survival.
For example, here’s a theory that should be investigated. Based on what we know about the immune response, natural immunity from COVID-19 should be more durable, more protective, and better for our communities than vaccine. Why? Natural immunity exposes the immune system to many different molecules, not just spike protein, making it more likely to sustain emergence of new variants. More durable immunity generates longer lasting herd immunity, reducing the size of subsequent disease spikes. At least that’s the theory.
How well does it work? We don’t really know.
Although other nations have found wisdom in this theory, the CDC has not permitted us to try it. Instead, the CDC stubbornly holds on to the universal vaccination idea, even vaccinating COVID survivors regardless of their antibody levels.
So how do we get out of this? We need data. We need answers to questions like what antibody levels indicate protective immunity? How long does natural immunity last? Is vaccine-induced immunity as protective natural immunity against variants? Can antibody levels be too high? What are the optimal antibody levels?
That’s why I’m excited about the Texas CARES Survey. This study sponsored by the UT Health Science Center at Houston, with testing by my friends and colleagues at Clinical Pathology Laboratories (CPL), promises to give us large cohort retrospective data on durability and magnitude of antibody responses after disease and/or vaccination, with matching outcomes. Although the study has met its initial enrollment goals, check back for results and more opportunities to participate.
Why has it taken so long to ask these questions?
- When We Lose Trust
There is a crisis of trust in America. One manifestation is in healthcare. For a century, the trust among Americans, their physicians, and institutions of public health built the most reliable healthcare system in history. Today that trust is being undermined, and the entire system is in danger of collapse. If we do not restore trust, we will suffer the reversal of a century’s gains in medicine.
The Youngest Science, a collection of essays by Dr. Lewis Thomas, traces medicine’s journey from pre-twentieth century practices into the evidence-based practices of today. Before this transformation, medicine was an unreliable mixture of traditional treatments like blood-letting and fanciful concoctions like snake oil tonic. Transparency, empirical evidence, and patient collaboration were absent.
Although there were many well intentioned physicians before the twentieth century, greedy hucksters and evil-doers thrived in this environment. Quacks with phony credentials wagoned into town hawking the one-and-only genuine medicinal potion that promised to cure whatever ailed you, often accompanied by craftily staged demonstrations. After selling as many worthless “cures” as possible, these predators escaped at night, leaving townsfolk poorer but in no better health. People naturally feared being duped again. Medicine could not progress in this environment.
In the twentieth century, trust changed all this. Beginning in 1906 with the Pure Food and Drug Act, the federal government developed institutions like the FDA, CDC and NIH to assure the safety and effectiveness of drugs and treatments. State governments licensed physicians and established standards of medical practice. Physicians organized, creating boards to prevent frauds from entering their ranks and abusing the trust of their profession. By the end of the last century, healthcare providers were among the most trusted professions in the nation. So much so that people were willing share intimate personal details with a stranger, as long as that stranger was a doctor or a nurse.
Now we see an erosion in the trust at the foundation of the youngest science. When trusted institutions like the CDC and FDA give incomplete or misleading statements, physicians lose a resource for reliable information. This quickly translates to a loss of the trust that bonds patients and physicians. As employers and political leaders displace physicians by claiming to be health experts, people are unsure who to believe. We’re back in the nineteenth century again.
It didn’t have to be this way. We could have leveraged medicine’s abundance of trust to lead us to recovery. Our trusted institutions could have given physicians the tools needed to make meaningful risk-benefit calculations for patients. But this would have required the acknowledgement that natural immunity is at least as good as vaccination in some COVID survivors, that vaccination is harmful to some individuals, and that vaccination does not prevent the spread of disease. We could have determined which groups receive the greatest benefit from vaccination, and which groups are most likely to suffer adverse effects. We could have guidance on measurable markers of immunity—what are the minimum protective antibody concentrations, and what levels are toxic—so that those at greatest risk of death from COVID-19 can determine whether they will benefit from vaccination or booster. We could have real data on adverse effects of vaccines by age and health status, and we could have balancing data on risk of death by SARS-CoV-2 infections. We are 18 months into the pandemic; we should have this information by now. Instead, our public health institutions have adopted an incredulously monolithic policy, saying universal vaccination is our only way out, even though we know this policy violates the oath of my profession: Do no harm.
Our trusted health institutions, like our trusted political institutions, have failed to communicate a clear, achievable objective for the pandemic. They have failed to demonstrate a connection between their policies and the achievement of this goal. As a result, we’ve lost trust. This crisis of trust has created a crisis of healthcare.
We must restore trust, together. The health of our nation is at stake.
- Is It Science?
How do you carve a statue of an elephant? Start with a block of stone and chip away everything that is not elephant. Science is like that. The elephant is truth; science is the chipping away. Scientists are the carvers, chiseling different parts of the stone block at once, testing and repeating each other’s findings, remodeling as new evidence emerges, and accepting the image that finally appears. Science is more verb than noun. It’s not the science; it’s just science.
You can’t predict what science will reveal hidden in the stone block. Even after the block is partially carved, you can’t be certain about important details that are still hidden from view. Science doesn’t reveal truth until scientists have finished their work, and that work cannot be rushed.
True science is open source. It invites questions, dissent, and transparency. True science is not condescending. True science can be understood by people with common intelligence. More than anything, true science is honest. When you identify misstatements, half-truths, or “believe me because I know better than you,” it doesn’t necessarily mean someone is trying to rob you, but it does necessarily mean you are not dealing with science.
And this is the point. Today’s intemperate rhetoric claiming to be science isn’t science at all.
I don’t have all the answers, but I recognize the absence of science in statements of leaders who say, “This is a pandemic of the unvaccinated.” The wisdom of universal vaccination, the benefits of vaccine mandates, the rejection of natural immunity have not been established scientifically. The use of ivermectin and hydroxychloroquine as prophylactics and early treatments have not been disproven scientifically. Yet there is an unrestrained rush to incorporate these ideas into the dogma of previously unimpeachable institutions and into our public health policies. It makes me sad. It makes me fearful for our future.
- O Goodness
The pandemic is a war, and our objective is survival. Many have asked what they can do to help the war effort. One way is to donate. I’m not asking for your money. I’m asking for your blood.
A chronic blood shortage has existed throughout the pandemic, but blood becomes even scarcer during surges. There are several reasons for this. People are reluctant to leave home. Work from home and distance learning reduces the yield of blood drives at businesses and universities. The health and safety measures necessitated by the pandemic reduce the rate at which donors who can be processed. All these factors result in less blood available for patients who need it.
Red blood cells are important because they carry the oxygen which fuels the body. Concentrations of red blood cells are given to patients who need a boost in their oxygen carrying capacity; sometimes this boost is lifesaving.
But it’s not as simple as taking blood from one person and giving it to another. Among other things, blood must be tested for compatibility. Every individual has a blood type, which corresponds to antigens on their red cells. Think of antigens as little self-destruct buttons on the cell surface. These buttons are imaginatively named A and B. There are four possible configurations of antigens, and these correspond to a person’s blood type. If you have only A antigens on your red cells, you are blood type A. If you have only B antigens only, you are blood type B. If you have both A and B antigens, you are blood type AB. And if you have no antigens, you are blood type O.
The buttons are pressed by antibodies floating in the liquid part of your blood. When the buttons are pressed, the red cells self-destructs (“hemolysis”). Don’t worry; your body can’t trigger the buttons on red cells made by your body. But your antibodies can trigger the destruction of red cells received during a transfusion. When transfused red cells self-destruct all at once, you have a reaction, and you could die. That’s why we want to know your blood type before transfusion. We need to make sure that the blood you get is compatible with you.
It turns out that if you are blood type A, you have B antibodies, meaning you can’t have any blood cells with B buttons. If you are blood type B, you have A antibodies, meaning you can’t have any blood cells with A buttons. If you are blood type AB, you don’t have any antibodies; you can get anybody’s blood (lucky you!). If you are blood type O, you have both A and B antibodies, so you can only get type O blood. But the cool thing about type O people is that there are no self-destruct buttons on their red cells. That’s why we call blood type O individuals “universal donors”—they can give their blood to anyone. In the blood bank world, O is good.
Type O blood is especially important in emergencies since there may not be time to test blood type before transfusion. At those times, type O blood is given immediately. O blood saves lives.
Our blood supply depends on the goodness of people. Since donation is the only source of blood, there’s just one reason blood is available for patients who need. It’s because someone took the time to give their blood voluntarily. About 45% of Americans are blood type O. If that’s you, you’re special. If that’s not you, we need your blood too. Having a supply of all blood types preserves type O blood for emergencies and for patients who can have no other type.
It may take a little extra time to donate during the pandemic, but your donation is needed now more than ever. It costs nothing but your time. It doesn’t matter if you’ve had COVID-19, been vaccinated, or not. Please consider making an appointment at a donation center now.
If you live in the Dallas-Fort Worth area, make an appointment here. Otherwise, find a blood center in your area here.
- How We Got Here
It was a scary time. When the first wave of COVID-19 swept through the nation in the spring of 2020, infection rates, hospitalization rates, and death rates climbed rapidly, and we didn’t know how high they would go. Nursing homes were especially ravaged. Once infected, more than 40% of people over 75 years old died. We were focused on keeping people alive, and we were committed to making sure that the sick had the resources for their best chance at survival. As hospitals filled up, our greatest fear was that people would die waiting for a ventilator. We determined to decrease the height of the wave by stretching out the time it would take to pass over us. Whether you agreed with the policy then, whether you agree with it now, that’s why we locked down, masked, and social distanced. We thought it was the best way to accomplish our objective of keeping people alive.
As the first wave passed, we relaxed a bit and found ways to feel normal again. We all stocked up on toilet paper. We tested small gatherings on Memorial Day and Independence Day. Those of us who survived (regrettably not all of us did) became convinced we could survive again. As the second wave of COVID-19 swept over us in the summer, we had new tools—tests, convalescent plasma, and drugs. And we had the promise of vaccines. If we could just hold on until the vaccines arrived, we would have a lifeboat that would save us from the virus and make things normal again. We all wished it would be so; it was not to be.
The second wave was devastating, infecting more people, and lasting longer than the first. Again, the elderly, the obese, and the diabetics were hardest hit, but more people survived infection this time. Mortality rates for those over 75 years old were cut in half—still too high, but better than before.
As the second wave passed and we entered the calm of fall, we began to see our vaccine saviors on the horizon. Applications were submitted to the FDA. But by now, the virus had mutated, and the more infectious alpha variant headed our way. This third wave, the largest and broadest of the three, proved that we had learned how to handle the virus. Death rates for infected individuals older than 75 dropped to 15%, about the same as Russian roulette. Still, more Americans died in the third wave than in the previous two combined.
As the alpha wave headed towards its crest, Pfizer-BioNTech received an EUA for its vaccine. People clambered for vaccination, especially the elderly and front-line health care workers. Moderna was authorized, then Janssen. Local health departments organized waiting lists, and people skipped work when they got the call for their turn. Operation Warp Speed put vaccines into arms in record time. And the alpha wave began to subside. There seemed to be an inverse correlation between vaccination rates and infection rates.
It was about this time, as lifeboats appeared on the horizon, that we lost our way. We stopped focusing on helping people survive, and we put our energy into pulling people into the lifeboats. We didn’t recognize that the boats were leaky, and that some people were better off where they were. We believed that vaccination would lead to eradication which would lead to freedom and our pre-pandemic lives again, but it wasn’t true. Even as the alpha wave receded, it became clear that the virus would be here to stay.
Yet we clung to the fantasy. We abandoned our initial objective of helping people live. Instead, we believed in the make-believe of universal vaccination—if we could just vaccinate everybody, the virus would leave earth. Nevermind that the vaccinated can pass the virus to others; at least they won’t be infectious for as long. Nevermind that the vaccinated get sick; at least they won’t die. Nevermind that some vaccinated died; their deaths are clearly the fault of the unvaccinated. Nevermind that vaccination doesn’t last very long, doesn’t prevent severe disease, and isn’t as good as natural immunity. Vaccinate! Vaccinate! And vaccinate again, with unauthorized boosters! Afterall, it’s a pandemic of the unvaccinated.
As the delta wave washes over us now, we must have the courage to believe what we see. Our vaccines are leaky, and they will not eradicate the virus. We cannot vaccinate our way back to our pre-pandemic lives. It’s time to change the paradigm.
We must return to our original objective of keeping people alive, and we must measure our actions, our public health policies, and our pandemic response against this objective. When we stop following the fairytale of universal vaccination, we can use vaccination as a tool to further our true objective of survival. We must develop other tools, prophylactics, and early treatments, and we must see whether any old tools can be repurposed to accomplish our objective.
We can defeat this pandemic if we change course, but the window of opportunity is closing. We must change course now.
- Quick Chart on Covid Mortality
This chart on Covid mortality provides perspective during the current spread of the delta variant. The CDC COVID Data Tracker shows weekly rates per 100,000 population for COVID-19 cases (CDC’s term for infections) and deaths since the outbreak of the pandemic. Selecting the dates corresponding to the peak death rate for each viral surge in the United States, I divided deaths by cases to approximate risk by age group:

While neither a comprehensive statistical analysis nor an entirely accurate calculation, this chart gives an idea of relative risk at important points in the pandemic. The delta wave has not peaked, so we may have not seen the highest death rates from the present surge. The risk of death for the elderly is consistently higher than for younger individuals, and, with few exceptions, age adjusted death rates have decreased in successive waves of the virus. Maximizing survival should be our objective as the pandemic continues.
- Leaky Vaccines
A perfect vaccine protects like a child’s immunity after chicken pox. It prevents future disease, prevents transmissions to others, and lasts for a very long time. Anything less is called a leaky vaccine. Let’s see how our current COVID vaccines stand up to each of these points:
- Prevent Future Disease. COVID vaccines don’t connect on this standard, and there are any number of reports that can show this. Just to pick one we haven’t discussed before, read the MMWR Early Release for August 24, 2021 which shows vaccine effectiveness dropped from 91% to 66% since the arrival of the delta variant, suggesting that vaccine is less protective against delta than pre-delta strains. But this data also shows that vaccine protection from disease was less than perfect even before delta. A perfect vaccine has effectiveness of 100%; our COVID vaccines never have.
- Prevent Transmission of Virus to Others. Another swing and a miss. To drive this point home, we need go no further than the CDC’s Recommendations for Fully Vaccinated Individuals, which states, “Preliminary evidence suggests that fully vaccinated people who do become infected with the Delta variant can be infectious and can spread the virus to others.” Still not convinced? A recent pre-print study from Vietnam demonstrates transmission between vaccinated healthcare workers. A perfect vaccine would prevent infection between vaccinated individuals; our COVID vaccines do not.
- Lasts for a Long Time. Strike three. Even though the vaccines have been available for less than a year, emerging data from Israel suggests that their effectiveness is already waning. My own antibodies lasted for less than five months. Vaccine-induced immunity doesn’t last very long.
Our COVID vaccines are leaky. So what? Just take a booster. And another. And another.
There are several problems with this reasoning. Here are three:
First, a false perception of protection leads to risky behavior. Maybe you’re young, and it doesn’t matter if you get a SARS-CoV-2 infection. Maybe you’re pregnant or elderly, and it does. When you believe that your vaccination protects you from future infection, you are more likely to ignore precautions that might protect your life, or the lives of others.
Second, leaky vaccines may stimulate the formation of more dangerous variants. The theory goes like this. The virus seeks a host. If vaccination reduces but doesn’t eliminate the available hosts, the virus feels evolutionary pressure to mutate into a form that will infect more people. Not everyone agrees with this idea, but there is enough evidence to at least consider this possibility.
Finally, leaky vaccines will not eradicate SARS-CoV-2, no matter how many boosters you take. Vaccination has eradicated exactly one human viral pathogen from the earth: smallpox. The smallpox vaccine was a perfect example of a perfect vaccine. It prevented disease. It prevented transmission. It lasted a lifetime. It eradicated the virus from the earth. And it took nearly 200 years. We cannot expect a leaky vaccine to produce the same results.
Maybe future vaccines won’t be as leaky as the ones we have now. Maybe we’ll even have a perfect COVID vaccine someday. We can hope. But until then, eradication is a pipedream. Instead, we must do all we can to protect the lives, the health, and the wellbeing of people while the virus is among us. We must learn to live with the virus.
- RSV
Respiratory Syncytial Virus (RSV) is a highly infectious virus that can lead to serious disease in children. The virus emerges each year roughly at the time school starts in the fall and subsides later in the spring. Midsummer RSV is unusual. Last year we did not see the typical rise in RSV, but this year the RSV surge started much earlier and is of much greater magnitude than normal. Our COVD-19 response has unintentionally increased children’s risk from RSV infection.

Respiratory syncytial virus, named because of the unique appearance of infected cells under the microscope. Lock downs, social distancing, and masking, whether voluntary or mandated, changed the rhythm of upper respiratory infections like RSV and Flu. Flu has yet to return; the last infection diagnosed in my practice was in May, 2020, at the tail of the 2019-2020 season. But RSV has returned with a vengeance, all over the world. To illustrate, look at this graph of RSV infections in Tokyo for the years 2017-2021. And this year’s cases are more severe than before. According to CDC, “Due to the reduced circulation of RSV during the winter months of 2020–2021, older infants and toddlers might now be at increased risk of severe RSV-associated illness since they have likely not had typical levels of exposure to RSV during the past 15 months.” You read that right. Anti-COVID measures, regardless how well-intentioned or how necessary, will cause more severe RSV disease in our children this year.
Just how severe is RSV? RSV is a major viral cause of death in children 5 years of age and younger, with mortality rates estimated between 0.5 and 1.7% in healthy U.S. children, but devastatingly higher in immunosuppressed children and in the children of the developing world. By comparison, the mortality risk for infants and children infected by SARS-CoV-2 is under 0.03%. RSV is a more serious risk to our kids than COVID.
There is no vaccine for RSV, and there is no treatment other than supportive care. Severe cases require ventilator support in a pediatric ICU. Most patients survive. According to the American Academy of Pediatrics Red Book, most kids are exposed to RSV by the age of 2, and reinfection is common.
Which brings us to the point. Even though RSV can cause a serious and deadly viral respiratory illness, the virus circulates among children. Children live with this virus. RSV prevention measures are targeted toward those at highest risk of death from the virus. Eradication of RSV is not the objective, and, as our experience in 2020 and 2021 suggests, may not even be desirable. The disruption of the seasonal viral pattern by implementation of COVID-19 precautions has increased the risk of sickness and death by RSV this year. Children derive benefits from natural exposure to RSV that may be important to their future survival.
We need to be aware that our actions during this pandemic can have consequences beyond what is in view. Homelessness, suicide, drug overdose, and now increased RSV–all unintended consequences of our public health policies. With this in mind, and the possibility of other unknown variables, we need to target our prevention efforts toward those at greatest danger. We must agree on a clear, sensible, and attainable objective. We must learn to live with the virus.
- Quick Chart on Current Covid Vaccines
The vaccine landscape became more complicated this week after FDA’s approval of COMIRNATY, the vaccine manufactured by Pfizer Inc. of New York for BioNTech Manufacturing of Mainz, Germany. I’ve prepared this chart to aid understanding of what’s approved, what’s authorized by EUA, and what’s neither approved nor authorized. I’ve also included the major warnings listed on the factsheets or prescribing information for each vaccine. A “No” in this section doesn’t necessarily mean that the complication cannot happen, since all authorized vaccines include the warning of other risks that are not listed.

An FDA approved vaccine is not available for injection as of this writing. We are learning that all these vaccines are “leaky.” Soon, I’ll post an article that breaks down what a leaky vaccine is and what that means for the pandemic.
- Did FDA Approve the Pfizer COVID Vaccine?
Yesterday’s FDA news release plainly says that the COVID vaccine that has been known as the Pfizer-BioNTech COVID-19 Vaccine has earned FDA approval and will now be known as COMIRNATY. So why were two letters issued by the FDA yesterday?
The approval letter, addressed to Amit Patel of BioNTech Manufacturing GmbH and delivered to Pfizer Inc. in New York, lists the conditions of approval, which include permission to the label the vaccine with the proprietary name COMIRNATY and permission to use the product to vaccinate individuals 16 years of age and older. The letter defers approval for use of the vaccine in individuals younger than 16 years of age, and it does not approve the administration of a booster shot.
On page 2, this letter states, “We did not refer your application to the Vaccines and Related Biological Products Advisory Committee because our review of information submitted in your BLA, including the clinical study design and trial results, did not raise concerns or controversial issues that would have benefited from an advisory committee discussion.” The letter then continues to outline deadlines for the submission of a list of outstanding items, some of which might be considered controversial. Here are a few that caught my eye:
- A study to evaluate whether the vaccine can safely and effectively be administered in a lower dose to individuals 12 to 29 years of age, due in 2023.
- A study to evaluate the safety of vaccine in pregnancy, including possible birth defects, due in 2025.
- Various studies to assess myocarditis and pericarditis after administration of vaccine, due between 2022 and 2026.
- A study to assess the safety and effectiveness of the vaccine in children 12-15 years of age (spring 2023), 6 months to <12 years of age (fall 2023), and children <6 months of age (summer 2024).
The approval letter also specifies deadlines for submission of final content of labeling “as soon as possible, but no later than 14 days from the date of this letter,” and proposed advertising and promotional labeling “before initial dissemination.”
The second letter, addressed to Ms. Elisa Harkins of Pfizer Inc. in Pennsylvania, is a revision of the Emergency Use Authorization for the Pfizer-BioNTech COVID-19 Vaccine. While this letter acknowledges Pfizer-BioNTech COVID-19 Vaccine and COMIRNATY are biologically equivalent and can be used interchangeably, it creates a legal distinction between them. This letter authorizes the continued use of Pfizer-BioNTech COVID-19 Vaccine and, when it is available, COMIRNATY in children between 12 and 15 years of age. It also authorizes administration of either vaccine in a third dose (“booster”) to certain immunocompromised individuals. It further permits Pfizer to continue to provide Pfizer-BioNTech COVID-19 Vaccine (but not COMIRNATY) to individuals 16 years and older under emergency use authorization until Pfizer’s inventory is consumed. All product labeled Pfizer-BioNTech COVID-19 Vaccine will “clearly and conspicuously state that it has not been approved or licensed by FDA.” Even though the vaccines are the same, if you get one labeled “Pfizer-BioNTech COVID-19 Vaccine”, you are not getting an approved vaccine; if you get the one labeled “COMIRNATY”, you may be, as long as you’re at least 16 years old and getting your first or second shot.
Yesterday I said that if the FDA short-circuited its rigorous approval process, the results would be deadly. I am not accusing the FDA of doing so; I am not an expert in FDA procedures. But I think we can agree that this approval is complicated, that some information we would all like to see is missing, and that much of that missing information won’t be available any time soon.
- What FDA Pfizer Approval Means
Today, the FDA approved the Pfizer COVID vaccine. This vaccine is the first of the three vaccines authorized under EUA to achieve this status. In this blog, I’ll highlight what this approval means. Obviously, this is just a first look at the information released by the FDA today. I’ve not studied the Full Prescribing Information in detail. There may be more changes that I have overlooked; I will update you on these as they become apparent.
First, let’s talk about what hasn’t changed.
- The vaccine has not changed. There have been no modifications to the vaccine. The vaccine that was injected before approval is the same as the vaccine given after approval.
- The warnings on the vaccine label have not changed. The Highlights of Prescribing Information issued with the vaccine approval have the same warnings that were listed for the pre-approval vaccine. These include acute allergic reactions (anaphylaxis), myocarditis and pericarditis, syncope (fainting), altered Immunocompetence, and limitation of effectiveness. Furthermore, Pfizer does not assure the safety of the vaccine in pregnancy or breast-feeding mothers.
- Vaccine experience is still limited. Although Pfizer updated its clinical trial data to include many more patients, and has expanded the observation period over more time, there are still no long-term clinical trials to study potential adverse effects this vaccine may have three, five, or ten years down the road.
So far, not much difference. What has changed?
- The vaccine is now called “COMIRNATY”. If anyone understands why they chose this name, please let me know. It’s not obvious to me.
- Approval does not include 12-15 year-olds. On May 10, the EUA for Pfizer vaccination was amended to include children down to 12 years of age. This vaccine is now approved for individuals 16 years and older. Children aged 12-15 may still receive the vaccination under a new reissued EUA.
- Removal of statement warning of unknown future risks. The previous Fact Sheet for Healthcare Providersincluded the following statement: “Additional adverse reactions, some of which may be serious, may become apparent with more widespread use of the Pfizer-BioNTech COVID-19 Vaccine.” This statement is not present in the Highlights of Prescribing Information issued with this approval. However, the Fact Sheet for Recipients and Caregivers still contains the following statement: “These may not be all the possible side effects of the vaccine. Serious and unexpected side effects may occur. The possible side effects of the vaccine are still being studied in clinical trials.”
- The Pfizer COVID Vaccine is no longer “unapproved”. This may not seem like much of a substantiative change, but the psychologic and motivational effect of this change will likely be significant. Those advocating vaccine resistance relished referring to COVID Vaccines as “experimental” because, technically, they were. Janssen and Moderna still are. You can’t call the Pfizer COVID vaccine “experimental” anymore because, technically, it’s not. This semantic change will embolden governments and employers to pursue vaccine mandates.
But this brings us to a few more things that haven’t changed. I have argued that vaccine mandates are wrong strategically, wrong temporally, and wrong ethically. There is nothing about FDA approval of vaccine that changes my opinion on this. Ethical physicians have a duty to speak out on issues affecting patient safety, even and especially during a pandemic.
The FDA can and has made mistakes in its approval process before. It will again. It may have in this instance; time will tell. But if the FDA has bowed to political pressure to short-circuit this approval, the long-term consequences will be deadly. Not just to the health and wellbeing of vaccine recipients, but also to the trust that is the cornerstone of America’s healthcare quality.
According to the AMA Code of Ethics, individuals must participate in their personal healthcare decisions through the process of informed consent which requires complete, clear, and honest disclosures of all known and potential risks and benefits. Approved vaccines are not exempted from this moral obligation. An article published recently in American Journal of Law & Medicine, states that “to be autonomous, decisions need to be based on full, accessible information and reached without coercion.” No matter how well intentioned, coercion by government or employer cannot be part of informed consent process. Not in the Land of the Free. Not in the Home of the Brave.
- Vaccine Mandates Are Wrong
I’ve argued that vaccine mandates are the wrong objective at the wrong time. In this article, I want to convince you that vaccine mandates are just plain wrong. Wrong—as in the opposite of right. That kind of wrong.
Wait, you say. The name of the website is BetterPathology.com. What gives a simple practitioner of pathology the right to lecture us on right and wrong?
Medical ethics is part of every physician’s education and training. There are gray areas to be sure, but there are also bright lines that separate ethical from unethical practice, and every doctor knows where these lines are. Every physician knows the elements of informed consent, and every doctor understands why the Tuskegee experiments were wrong. There are aspects of vaccine mandates that should be troubling to all ethical physicians and all ethical Americans.
To the extent they are able, patients must participate in medical decisions. Informed consent requires a doctor to explain in understandable language the risks and benefits of a recommended treatment, the risks and benefits of alternative treatments, and the risks and benefits of doing nothing. It’s one thing to recommend the risks of a therapy when a patient’s natural disease leaves no other options. It’s quite another thing to recommend a vaccine when the most significant consequence of refusal is job loss. Threatening a young person to accept the risks of vaccine against his will smacks of Don Corleone’s “offer he can’t refuse.” Coerced consent is unethical.
Once we lose the freedom to evaluate and choose risks for ourselves, we lose the liberties at the foundation of our nation. When vaccines are mandated by a government or an employer, the right to choose what we want to put in our bodies is taken away from us. When we lose this liberty, how long until we also lose the freedom to associate with those we wish, to worship as we please, to speak our minds, or to choose which path we wish for our lives?
Vaccine mandates stigmatize dissent and erode individual liberty, separating society into vaccinated people and unvaccinated people. The vaccinated will have freedoms while the unvaccinated will be denied freedoms. Vaccinated individuals will have the freedom to eat at any lunch counter; unvaccinated folk will be seated outside in the back. The vaccinated will be able to watch the ballgame from box seats; the unvaccinated will be forced into designated sections in the outfield. There will be separate water fountains for vaccinated people and unvaccinated people. There will be separate entrances into public establishments. Vaccinated people will have unlimited job opportunities while the unvaccinated will find employment prospects limited. The vaccinated will enjoy unrestricted travel in the mode and style of their choosing; the unvaccinated will have to ride in the back of the bus, partitioned by a plexiglass shield. Ethical Americans, like ethical physicians, know the immorality of this type of irrational segregation which is based on the false premise that only the unvaccinated can make others sick.
There have been some ugly chapters in our history. Let’s not write a new one.
- Vaccination Card Folly
Do Vaccination Cards Keep Us Safe?
Before I answer that question, I’d like to tell a personal story. I took a single dose Janssen vaccine March 15, 2021. I measured my spike protein antibodies on May 20 to make sure that the vaccine worked; my test was positive with an index level of 1.4. Last Thursday, August 12, I measured my antibodies again. They were negative. I have a vaccination card that I can use to sit in a New York City restaurant, attend a concert at SFJAZZ, live on a university campus, or work at a hospital that has mandated vaccines. Even if H.R. 4980 becomes law, I will be able to travel on an airplane in the United States. Yet not even five months since my vaccination, there is no longer evidence of antibody-based immunity in my blood.
My story is another example of the folly of making universal vaccination the primary objective of the pandemic response. Vaccine mandates by restaurants, employers, airlines, colleges, and entertainment venues are based on the flawed assumption that vaccinated people are safe, clean, and not dangerous to others. There is undeniable evidence that breakthrough infections occur, that the vaccinated can spread the disease, and that vaccinated individuals can die of the disease. It’s becoming clear that eradication is no longer possible.
There is also mounting evidence that vaccines are associated with significant side effects that affect the health and wellbeing of individuals. Expect more evidence to emerge. We do not yet know the whole story.
I don’t have all the answers—nobody does. Our understanding of both the virus and the vaccines are so far from complete that it’s impossible for anyone to make sweeping recommendations, no matter their position, no matter their intelligence. But there is one thing we know for sure. Clear objectives drive sound decisions. Before we can win this war, we must agree on a sensible objective.
Our desired outcome should be keeping as many people alive as possible. The life, health, and wellbeing of all individuals are paramount. When we give primacy to vaccination status, we lose sight of our noble objective, and we divide people into uncooperating groups. To the extent that vaccines further our objective, we should use them. To the extent that early treatments further this objective, we should use them. To the extent that therapies and treatment protocols have not been fully studied by science, we should fund studies publicly. Although we can count on the free market to sponsor research when there’s the prospect of a large profit, wouldn’t it be a shame to overlook regimens that can keep people alive just because there’s no money to be made? But we should never confuse any of these tools with our primary objective. We must allow people to make choices, and we must allow doctors to make personalized decisions in the best interest of individual patients.
Eradication is no longer possible, but survival is. We must learn to live with the virus. Have faith. Have courage.
- Common Sense
As SARS-CoV-2 infections are increasing and some parts of the country are experiencing their highest rates of the pandemic, we face a medical shortage. In Texas, the supply of staffed hospital beds is shrinking, and some communities are out of ICU beds. Staffing shortages are becoming critical. Is this the time to fire doctors, nurses, and other healthcare professionals for refusing a COVID vaccine?
Many people feel sick after a COVID vaccination, and some of those people won’t be able to come to work. The Janssen vaccine isn’t fully effective for two weeks after the shot. It takes five weeks for Pfizer and six for Moderna. Meanwhile, hospitals are short on beds, and even shorter on staff. Which will save more lives—fully vaccinated healthcare workers or staffed hospital beds?
The healthcare community has managed COVID surges without vaccine before, and we can do it again. The universal vaccination of healthcare workers achieves no benefit that justifies the violation of individual liberty required to achieve this goal. You may disagree with me. We should have that debate.
But right now, those of us who work at hospitals have our hands full taking care of COVID patients. Can we talk about this later?
- Updates, Questions, Present, and Future
A lot changed in pandemic landscape last week. This blog outlines those changes and highlights important unanswered questions.
- The surge of delta virus infections continues across the country. Several weeks ago, I announced that the pandemic is over. That statement requires revision. Maybe the pandemic of alpha virus was over then, but the epidemic of delta virus is here now. Delta virus is the overwhelming variant in the U.S. with parts of the country (Florida, Hawaii, and Louisiana) experiencing their highest cases of the entire pandemic.
- Deaths are up, but still low. Unfortunately, it’s no longer the case that deaths are at the lowest level of the pandemic. Deaths have increased with the current surge of delta virus. Although even one death is too many, it is reassuring to see that deaths are not at levels seen during the winter surge, and that deaths have increased at a lower rate than infections during the current surge. As with the previous two surges, older individuals are at great risk than younger individuals. Based on data from the CDC COVID Data Tracker, COVID-19 deaths per ten million Americans during the week of July 24, 2021, were:
- 2 for individuals between 18 and 29 years-old
- 5 for individuals between 30 and 39 years-old
- 14 for individuals between 40 and 49 years-old
- 22 for individuals between 50 and 64 years-old
- 39 for individuals between 65 and 74 years-old
- 101 for individuals aged 75 years and older.
- New testing recommendations for COVID vaccinated individuals. The CDC has changed its testing recommendations for vaccinated individuals who have had an exposure to someone with SARS-CoV-2 infection. An exposure is still defined as contact of less than 6 feet for more than 15 minutes when one or both individuals are not wearing a mask. Before this change, COVID vaccinated individuals were asked to test only if symptoms developed. Now a SARS-CoV-2 test is recommended for COVID vaccinated individuals 3 to 5 days after the exposure, and the exposed individual should wear a mask indoors for up to 14 days until a negative result is obtained.
As individuals decide how to mitigate personal risk of death from COVID-19, the following information on the CDC COVID Data Tracker would help people make better decisions:
- Reinfection rates and deaths among previously infected individuals. Contrary to CDC recommendations, I believe vaccination of COVID survivors is a risk without benefit. We could know the answer for sure if cases and deaths in the CDC COVID Data Tracker were stratified by previous infection status. If unvaccinated people with previous infections have low infection and death rates, we could conclude that previous infection provides protection from COVID-19.
- Infection rates and deaths among previously vaccinated individuals. This data exists, but not on the CDC COVID Data Tracker. We could have a better understanding of the risk of breakthrough and serious disease if the CDC compiled and published this information beside the other important and helpful information on its website.
- Vaccination complication rates by age and severity. This information is essential to a risk/benefit analysis of COVID vaccination, but this data is especially difficult to compile for several reasons. First, not all adverse effects report on VAERS are truly vaccine related. Second, not all vaccine related adverse effects are reported on VAERS. Finally, not all adverse effects caused by vaccine are recognized as such. Delayed effects may never be flagged as vaccine related. It may take years to ever sort out this problem. The best we can do now is look at the vaccine warnings (see Pfizer, Moderna, Janssen), including the warning that “additional adverse reactions, some of which may be serious, may become apparent with more widespread use”. We must continue to expect unknown consequences.
We are in our second year of the pandemic, and we have some experience to help us understand what’s coming. The U.S. is experiencing its third surge of SARS-CoV-2 infections. The first surge was associated with the original form of the virus. The second surge coincided with the replacement of the original form by alpha variant. The current surge began as the wave of delta variant replaced alpha. Will it be the case that a surge will be experienced time a more infectious variant replaces its predecessor? Could be.
- Staying Alive
If anything is sacred, the human body is sacred.
― Walt Whitman
How should we define victory in the war on the pandemic? My vision may surprise you. I think our objective should be not dying. Death rates should be our success metric, and the preservation of our institutions and freedoms our goal. We can accomplish this by making smart individual decisions, not sweeping collective ones. We cannot allow our society to be fractured into camps of the vaccinated and unvaccinated.
The universal vaccination mandates sweeping across our nation now are more dangerous than the current wave of SARS-CoV-2 infections. Don’t believe me? Check out the CDC’s COVID Data Tracker. Deaths from COVID-19 are at their lowest levels since the pandemic began. Yet on pain of job loss, we are pushing vaccines into the arms of our young who have the most to lose and least to gain.
Don’t get me wrong. Vaccination is an important tool in our effort to save people from dying of COVID-19. Those at greatest risk—the old, the obese, the diabetics—should strongly consider vaccination for their own safety. Vaccines also reduce the spread of COVID-19 within a community. When vaccines became available in late December, community infection rates declined as vaccination rates went up. But that doesn’t mean that vaccination is in the best interest of every individual.
Wait, I hear you say, we must vaccinate everybody to contain breakthrough and stop the spread of the virus. Especially hospital workers—I want to know that people taking care of me are vaccinated so they won’t make me sick. Nice theory, but where’s the data that supports the idea that vaccinated people can’t make you sick, that vaccines contain breakthrough and stop the spread of the disease? I’ve looked; I can’t find it. If you have it, please share it with me.
I see data that supports the opposite theory. In last Friday’s Morbidity and Mortality Weekly Report (MMWR), the CDC reported a SARS-CoV-2 outbreak in a highly vaccinated community. Some were shocked to learn that three-quarters of these cases occurred in fully vaccinated individuals, that the viral loads between vaccinated and unvaccinated individuals were identical, and that four out of five patients sick enough to be hospitalized were fully vaccinated. This report supports one of the points made last week: vaccination doesn’t prevent COVID-19. Breakthrough cases occur, and the vaccinated can spread the virus. Universal vaccination will fail as a containment strategy.
But, you persist, we have to vaccinate everybody before new variants emerge that will be even more dangerous. After all, you say, 90% of the virus in the reported outbreak were delta variant. True, this outbreak was mostly delta variant, but delta variant is now the dominant variant in the U. S. because of its higher transmissibility, just like alpha variant replaced original SARS-CoV-2 earlier in the year. Where is the evidence that universal vaccination prevents formation of more dangerous variants? Again, I’ve looked, and I don’t find it. If you have it, please share it with me.
Infectious disease orthodoxy says the opposite. Indiscriminate use of anti-biologic agents pressure pathogens to mutate, increasing their virulence. Doctors are reprimanded for treating viral illnesses with antibacterial agents (“antibiotics”) because they have potential for more harm than good. The same is true for vaccines designed to prevent infections by viruses that easily mutate. That’s one reason we don’t have vaccines for the common cold—the target moves too quickly, and infection is not that dangerous to most people. Universal vaccination will fail to prevent emergence of variants.
If universal vaccination becomes our objective in the war against the pandemic, deaths may increase, surges may continue, and more dangerous variants may emerge, but won’t we feel good about our vaccination rates? The pandemic has an enemy; it’s not the unvaccinated.
There is another way. Allow doctors to make individualized decisions for treatment and vaccination in the best interest of each patient. If we do all we can to help those at risk, deaths will continue to go down. The virus may never go away, but we can learn to live with it. We can also preserve our institutions and freedoms, and we can stop dividing people. We can stay alive.
- A Pandemic of the Unvaccinated?
During a White House press briefing last week, Dr. Rochelle Walensky, the director of the CDC, declared, “This is becoming a pandemic of the unvaccinated.” She continued, “And our biggest concern is that we are going to continue to see preventable cases, hospitalizations, and, sadly, deaths among the unvaccinated.” Is there a rational basis to allow our war against the pandemic to devolve into a fight between vaccinated and unvaccinated citizens? In this blog, I will use data found at the CDC’s website to outline what we know and what we don’t about vaccinations, infections, disease, and death.
What we know:
- SARS-CoV-2 infections have increased recently. It’s easy to see this point from the CDC’s COVID Data Tracker. Play with the graph a little. By clicking any of the boxes (sex, age, ethnicity) under “Cases” on the upper left, you’ll see case trends of the entire pandemic. Pass your cursor along the horizontal axis, and you’ll see the rate of cases each week of the pandemic. The number of cases bumped up in the first two weeks of July. But the recent increase is not yet close to levels of the surge last winter.
- Deaths from COVID-19 are still going down. Using the same graph, click on any of the boxes under “Deaths” on the upper right. The last week deaths increased was May 8, and then only by a little bit. There has not been a spike in COVID deaths since the winter surge. Even as infections increased recently, deaths have not.
- Risk of death from COVID-19 increases with age. Now look specifically at deaths by age. Move your cursor along the horizontal axis and pay attention to the death rate as age increases. It’s the old who die from COVID-19, not the young.
- Vaccination rates are highest among those at greatest risk of death from COVID-19. Now study another chart from the CDC’s COVID Data Tracker. Notice that in increasing age groups, more and more people are at least partially vaccinated, more than 90% among 65–74 year-olds. The old, who have the greatest risk of death from COVID-19, also have the highest vaccination rates.
- Vaccination does not prevent COVID-19. Breakthrough cases occur, and vaccinated individuals can spread the disease. This last point is well known by everyone who follows Texas politics.
- Community vaccination rates correlate with reduction in COVID-19 spread. For this point, study the CDC’s vaccination vs. covid heat map, showing lower rates of COVID-19 where vaccination rates are higher and vice versa. This is the data Dr. Walensky points to when saying “This is becoming a pandemic of the unvaccinated.” However, unless she has private data not on the website, I do not see a similar correlation between deaths or even hospitalizations. Death rates continue to decline, even among the unvaccinated.
- Vaccination is associated with significant adverse effects, including death. Guillain-Barré Syndrome, inflammation of the heart, blood clots, anaphylaxis—and these are just the labelled complications. Expect more immune-mediated vaccine complications to emerge in the future.
There are some things we don’t know, and we don’t know them because we don’t yet have good data. For example, the CDC tracks COVID-19 deaths by sex, age, and ethnicity, but not by vaccination status. That information would be very helpful to individuals deciding whether to take a vaccine. So would age-adjusted vaccine complication rates. The absence of such data makes it difficult-to-impossible for young people to determine their personal risk-benefit ratios for vaccination. The VAERS website is good for its intended purpose as a reporting site for adverse events, but the data must be mined and analyzed to be meaningful.
Good data is simply hard to come by. Last week, Sir Patrick Vallance said in a press conference that 60% of hospitalized COVID-19 patients in the UK are fully vaccinated. Later, he tweeted a correction, saying exactly the opposite. The trouble is that it’s impossible to validate either statement with reliable, publicly available data.
Science is a process, not a product. For science to work, conventional wisdom must be questioned. It is always okay to ask, “Why should I believe this?” Dissent is a natural byproduct of science. But dogmatism, coercion, ridicule, hyperbole, and fearmongering have no place among real scientists. Not even the director of the CDC.
- A New Vaccine Warning: Guillain-Barré Syndrome
Last week, the FDA added a new statement to the Janssen vaccine Factsheet for Healthcare Providers, warning of an increased incidence of Guillain-Barré Syndrome among vaccine recipients. This warning was issued after cases in India and the United Kingdom were published in the Annals of Neurology. Although the warning only applies to the Janssen vaccine, at least one case has also been reported following Pfizer vaccination.
Guillain-Barré Syndrome is a condition in which the immune system attacks peripheral nerves, the nerves responsible for sending signals for motion and sensation between the body and the brain, resulting in pain and weakness, and in severe cases, paralysis and death. Although most people recover, symptoms may linger for a long time. Guillain-Barré Syndrome is triggered by various conditions that cause inflammation, including infection, surgery, trauma, and cancer. Rarely influenza and childhood vaccines have been associated with Guillain-Barré Syndrome.
Guillain-Barré Syndrome was identified as a complication of COVID-19 early in the pandemic. Subsequent studies demonstrate that these cases are “not due to a direct attack of the virus, but rather to an immunological reaction to the virus.” Now we learn this long-recognized complication of COVID-19 can also be an adverse effect of a COVID vaccine.
The warning for Guillain-Barré Syndrome is the third FDA statement of an immune mediated vaccine complication, adding to the precautions previously issued for myocarditis and clotting disorders. Interestingly, myocarditis and clotting disorders have also been recognized as complications of COVID-19.
It’s becoming increasingly clear that COVID-19 has two separate disease pathways. The first is the direct effect of the virus. The second is the response of our immune system to the virus. Vaccines intentionally stimulate this immune response. Is it surprising that adverse vaccine effects overlap with COVID-19? Expect more examples of autoimmune complications of COVID vaccines.
- COVID and Autoimmune Disease
Some individuals infected by SARS-CoV-2 experience brain damage. Although it sounds like science fiction, “COVID brain fog” describes a very real condition in which infected patients experience memory loss, strokes, and other nervous system lesions. How can this happen?
In an article published last week in Nature, Michael Marshall, a free-lance science journalist from the U.K., describes the current areas of research into the causes of this condition. One possible mechanism is autoimmune disease.
The immune system’s job is to protect the body from agents of disease (“pathogens”) without damaging the body’s own cells. Like the military guarding the border of a sovereign nation, the constituents of the immune system carry lethal weapons meant to destroy an invading enemy. But what if the military can’t tell the difference between friend and foe? Those lethal weapons might be unleashed on its own people, and the citizens of that nation would be at risk of harm from their own government. Let’s say for example that the U.S. learned all its enemies wear red hats. If the army was ordered to seek and destroy anyone wearing a red hat, many innocent Americans unwittingly wearing red hats could be killed in an effect to stamp out a threat to our nation.
The immune system works by learning something about the pathogens that threaten the body—not the color hats they wear, but the shape and composition of molecules on the invaders. When the shape and composition of those molecules are similar enough to the shape and composition of molecules on the cells in our own body, the immune system can’t tell the difference, and it attacks us. That’s autoimmune disease.
Autoimmune disease is highly individualized. Although we lump these diseases into categories ranging from lupus to rheumatoid arthritis, each person with an autoimmune disease has a disease that’s uniquely his or her own. There’s a lot of overlap, but no two individuals have exactly the same disease manifestations.
There are many examples of autoimmune disease targeting specific organs. Hashimoto’s thyroiditis is a disease in which the immune system targets the thyroid gland. In Crohn’s disease the immune system targets the cells of the gastrointestinal tract. Multiple sclerosis is an autoimmune disease of the central nervous system. COVID brain fog may also be, at least in part, an autoimmune disease of the central nervous system in which an immune system primed to destroy SARS-CoV-2 causes collateral damage to the brain.
If that’s the case, we have yet another reason to avoid COVID-19. But we may also want to avoid stimulating the immune system to fight SARS-CoV-2, which is precisely the goal of a COVID vaccination. We know that everyone who has had COVID-19 develops antibodies to the viral spike protein. We also know that everyone who has received a COVID vaccine develops antibodies to the same viral spike protein. What if these are the autoantibodies associated with COVID brain fog?
Although there is no proof this is the case, there is evidence suggesting that the idea is plausible. Last week, we learned that vaccines may cause myocarditis and pericarditis, essentially an autoimmune disease affecting the heart. VITT, a condition in which vaccination causes blood clots, is also immune mediated. We must consider the possibility that stimulation of immunity against viral spike proteins causes autoimmune disease in some vaccine recipients.
As we connect more dots, an image emerges from the haze of the pandemic. As the picture becomes clearer, will we have the courage to believe what we see?
- More Vaccine Complications
We have warned of the dangers of unforeseen consequences inherent in medical therapies and procedures that have not been thoroughly tested. All COVID vaccines are in this category since they are only available in the U.S. are under Emergency Use Authorization. None has been approved by the FDA.
Information about vaccine complications is slowly emerging. First, we learned of the 10x higher incidence of anaphylaxis from mRNA vaccines compared to other vaccine types. Then we learned of a new clotting disorder caused by vaccine called VITT. Last week, the FDA required a new statement in Pfizer and Moderna Factsheets for Healthcare Providers warning that certain cardiac disorders, including myocarditis and pericarditis, may be caused by mRNA vaccines.
In the pathology world, adding “-itis” to the end of a word simply means inflammation. So, myocarditis is inflammation of muscle (“myo-”) of the heart (“card”), and pericarditis is inflammation of the sac around (“peri-”) the heart. By themselves these words are vague and do not say what that inflammation means to a person. Myocarditis can be mild and go away on its own, or it can be severe and cause the heart to stop beating. Similarly, mild pericarditis is a common finding in many disease processes, but pericarditis can become so severe that it restricts the movement of the heart, a condition called “cardiac tamponade” which can be deadly.
These vaccine complications tend to occur in young people who receive mRNA vaccines (Pfizer and Moderna, but not Janssen), especially when there is an underlying cardiac condition. The trouble is that this vaccine complication may be the first sign of an underlying cardiac condition, since “in this younger population, coronary events are less likely to be a source of these symptoms.” Does this make the vaccine unsafe for adolescents and young adults? The CDC says no; I’m not so sure.
It’s noteworthy that none of these complications—not anaphylaxis, not VITT, and not inflammatory heart conditions—were included in data submitted to FDA for initial authorization. We are learning as we go. Quite literally, if you take a COVID vaccine, you are part of a study of the long-term effects of that vaccine on humans. There may be compelling reasons for a person to take a vaccine, ranging from personal health benefits to scientific altruism. But just as compelling may be the reasons a person chooses not to take a vaccine. We should not coerce these decisions, we should not ridicule these decisions, and we should not penalize individuals for these decisions.
We simply don’t know all the long-term consequences of the COVID vaccines. But if history is any guide, there will be unintended consequences that may make the “smart people” of today look foolish in the future.
- Which Vaccine Causes the Greatest Antibody Response?
It’s not even close. In terms of generating the highest S-antibody response, Moderna is the clear winner. Pfizer comes in second, and Janssen (Johnson & Johnson) finishes in last place. Here’s the data that backs this up.
The same volunteers we tested to figure out antibodies after vaccination and disease were separated by vaccine type and evidence of infection. Evidence of infection includes either a positive SARS-CoV-2 test during the pandemic or the unexpected presence of N-antibodies. We did not count two individuals who had only one dose of mRNA vaccine, nor did we include people who had both vaccine and infection. Then we measured the antibody levels of the individuals in each group. Here’s what we found:
Vaccine Low High Average Moderna 8.4 9.1 8.7 Pfizer 4.2 7.6 6.2 Janssen 1.4 3.9 2.6 Clearly, Moderna vaccine stimulates the highest antibody response. Then we graphed the antibody response caused by vaccine compared to the immune response of infection.

Previous infection is better than the Janssen vaccine and nearly as good as the Pfizer vaccine. If we eliminate those overachieving Moderna people, we get a chart that looks like this:
Immunity Source Low High Average Pfizer or Janssen 1.4 7.6 6.2 COVID 1.2 8.4 4.3 Graphically, the data looks like this:

It’s nearly identical.
Let me summarize the findings and restate the question that’s been puzzling me for weeks. Two of the three vaccines authorized in the U.S. stimulate S-antibody levels that are no better than SARS-CoV-2 infection. Yet the CDC still insists that infected individuals be vaccinated with any of the three authorized vaccines, even if the person starts out with S-antibody levels at least as high as the expected levels resulting from vaccination. Why?
Let me be clear. I’m not asking whether a person who has not had COVID should be vaccinated. That’s a legitimate question that deserves more than knee-jerk consideration, but it’s not the question I’m asking here. I’m asking why vaccination is in the best interest of a person who has already been infected? Maybe the answer is obvious to you; if so, please help me understand. It doesn’t make sense to me.
Last time, I asked you to consider that the answer may be in the prioritization of population health over individual health. This time I ask you to consider something else. When things don’t make sense to me, I have a snarky, cynical side that asks, “Who’s profiting?”
Something to think about.
- The Delta Variant
The Delta Variant is one of several new strains of SARS-CoV-2 recently added the variant zoo. Why has this new variant received so much attention lately, and why are we referring to variants with Greek letters now?
The CDC still groups variants into categories of High Consequence, Concern, and Interest. Thankfully, there are still no Variants of High Consequence. The WHO has assigned Greek letters to certain variants to aid in communication. The Delta Variant, B.1.671.2, is a new entry on the list of Variants of Concern. Three cousins of the Delta Variant, B.1.671, B.1.671.1 and B.1.671.3 are now on the Variants of Interest list. All these new strains originated in India.
What makes Delta different? It’s the first addition to the Variant of Concern list since April, and it’s prevalence in the U.S.is increasing. Although it’s not nearly as prevalent as the Alpha Variant, aka the U.K. Variant, B.1.1.7 which we first learned about last December, some reports suggest that the Delta Variant is even more easily transmitted, meaning that it may soon replace the Alpha Variant as the most common form in the U.S. The Delta Variant shows some resistance to treatments, although not more than other variants. It does not escape detection by tests, and S-antibodies, either from disease or vaccine, seem to provide immune protection. The Delta Variant is just the ‘new kid on the block’; we need to take this in stride.
I’ve updated variant reference tables, sorted by U.S. prevalence.
Variants of Concern Variant WHO Label First Detection Current U.S. Prevalence Increased Transmission Increased Severity Reduced Detection by Tests Resistance to Treatment B.1.1.7 Alpha UK 69.7% 50% ● P.1 Gamma Japan/Brasil 8.4% ● B.1.617.2 Delta India 2.7% 140% ● B.1.351 Beta South Africa 0.7% 50% ● B.1.429 Epsilon California 0.6% 20% ● B.1.427 Epsilon California 0.4% 20% ● Variants of Interest Variant WHO Label First Detection Current U.S. Prevalence Increased Transmission Increased Severity Reduced Detection by Tests Resistance to Treatment B.1.526 Iota New York 5.0% ● B.1.526.1 New York 2.5% ● B.1.525 Eta UK/Nigeria 0.1% ● B.1.617.1 Kappa India 0.1% ● P.2 Zeta Brazil 0.0% ● B.1.617 India 0.0% ● B.1.617.3 India 0.0% ● - Vaccinate the Previously Infected? A Risk without Benefit
Vaccination of the previously infected is a risk without benefit because there’s no significant difference between S-antibody levels stimulated by SARS-CoV-2 infection when compared with vaccine.
Using the same group of volunteers from our study to determine antibody types stimulated by vaccine and/or COVID, we measured the level of S-antibodies in the people who had them. To make the comparison fair we did not consider the people who were both vaccinated and infected; instead, we only counted people who were vaccinated but had no evidence of disease, and we compared them to unvaccinated people with evidence of infection. Here’s what we found:
Individuals Low High Average Vaccine 17 1.4 9.1 6.6 COVID 8 1.2 8.3 4.2 There were 17 people vaccinated without disease. Their S-antibody levels ranged from 1.4 to 9.1 with an average of 6.6. There were 8 unvaccinated individuals with evidence of infection. That evidence could with be a positive SARS-CoV-2 test sometime during the pandemic, a positive N-antibody test, or both. Their S-antibody levels ranged from 1.2 to 8.3 with an average of 4.2. Any level above 1 is considered positive.
Graphically, the data looks like this:

Give a slight edge to vaccine, but really the difference between the two groups is negligible. The COVID group includes a couple who previously had asymptomatic infections, implying that even asymptomatic infections cause the formation of S-antibodies just like vaccines.
Which causes us to return to the question we asked in early May. Why vaccinate COVID survivors? I still see no evidence for doing so, but there are reasons for not vaccinating previously infected people. Our study includes two previously infected people who took the first dose of an mRNA vaccine and experienced vaccine complications so severe that they couldn’t take the second dose. One of the two developed a debilitating condition that has not yet resolved and may persist for life. Through June 7, 2021, VAERS received 5,208 reports of death associated with vaccine administration in the U.S. Clearly the vaccine did not cause every reported death, but just as clearly, the vaccine death rate is greater than zero. Death is the most serious of complications. There are more common but less serious complications that range from inconvenience to discomfort to debilitation. If there is no benefit, why take a risk? That’s why my advice is that previously infected people should not be vaccinated without a compelling personal indication.
Some researchers are beginning to agree with me. As early as February, a study subsequently published in Nature suggested that a second dose of mRNA vaccine is unnecessary for people previously infected by SARS-CoV-2. More recently, a pre-publication report of a study conducted at the Cleveland Clinic concludes that vaccinating individuals who have had SARS-CoV-2 infections has no benefit.
So why does the CDC still adamantly insist that COVID-19 survivors be vaccinated? The answer lies in perspective. The vaccination rate in a community is the single greatest factor in controlling the spread of disease and achieving the goal of herd immunity, which has already been reached in many parts of the country. If you prioritize the good of the population over the good of any individual, then you advocate for universal vaccination even when the vaccine has no benefit, or worse yet, may cause harm to individuals.
That is not my focus as a physician. My focus is the individual, the patient in front of me. Health care is not a commodity that can be mass-produced without hurting individuals. I have urged that vaccine decisions be made individually, not collectively, and I continue to do so. I believe that the people with greatest risk of unnecessary harm from vaccine are the previously infected and the young.
The suggestion that even asymptomatic infections cause the formation of S-antibodies has implications in the ongoing debate regarding the vaccination of children, the group most likely to have asymptomatic infection. During this debate, we must first resolve whether our priority is the population as a whole or the individual boys and girls subject to vaccination. We may reach different conclusions depending on the priority we choose.
Here’s an idea. Why not check S-antibody levels before vaccination? Something to think about.
- THE PANDEMIC IS OVER
What gives a Texas pathologist practicing in a suburban community the right to declare THE PANDEMIC IS OVER in screaming headlines? Shouldn’t such a pronouncement come from an official institution like the NIH or the CDC or the WHO or a prestigious university? Read on, I’ll tell you.
The graph of the number of positive tests resulted each week by the laboratory where I practice gives you a fair image of the pandemic in my community:

There were two waves, a small one last summer and a bigger one in the winter. But since the end of February, the number of positive tests has been low and constant. Positive tests have not disappeared, but the rate of positives is not changing. Search for rates in your community, and I bet you’ll find a similar graph.
Recall that epidemic means an increasing number of cases in a community, and that pandemic means an epidemic all over the world. From the graphs it’s obvious that the number of cases is not changing, and it hasn’t been for several months. If there’s no epidemic in my community and there’s no epidemic in your community, then there’s no more pandemic. The pandemic is over.
The graphs also tell us that the virus is still here, and probably will be for a long time, maybe forever. Epidemiologists call this the endemic rate—the rate of disease that is always present in a population. People will still get sick, and some may even die, but it’s no longer an epidemic. We reached herd immunity more quickly than many “experts” predicted.
So now what? We have to learn to live with the virus. Know your immunity status. If you are not immune, continue COVID precautions if you wish to avoid contracting the virus. The pandemic may be over, but the virus and its variants will be with us for a long time.
- Antibodies after Vaccination and Disease
Last time, we built a mental model of the SARS-CoV-2 virus and used that model to make predictions of antibody test results. This time we will see how that model squares against real-world observations.
Here’s the table we created last time:
Infected Uninfected Vaccinated S+ N+ S+ N- Unvaccinated S+ N+ S- N- With their permission, I tested more than 40 individuals who fit into one of the four categories. Here’s what I found:
Infected Uninfected Vaccinated 4 S+ N+
7 S+ N-17 S+ N-
3 S+ N+Unvaccinated 4 S+ N+
2 S+ N-4 S- N-
2 S+ N+Previously Infected and Vaccinated. There were eleven people in this category, but only 4 had both the S- and N-antibodies that our model predicted. Surprisingly, nearly two thirds of the people in this group lacked N-antibodies. This is not what our model predicted. It seems some people may not form N-antibodies. Let’s keep looking.
Previously Infected but Unvaccinated. There were six people in this category. Four had both S-antibodies and N-antibodies, but two had only S-antibodies. Again, we’re missing some of the N-antibodies predicted by our model. What’s going on here? I’ll offer some speculations later.
Vaccinated without Known Infection. There were twenty people in this category, and all but three of these individuals had the expected S+ N- antibody pattern. All outliers were S+ N+, suggesting they had asymptomatic infections sometime during the pandemic. Is this suggestion reasonable? I think so. During the pandemic we tested healthy patients before elective surgeries and found a significant number of asymptomatic infections, so we know this can happen.
Unvaccinated without Known Infection. There were initially five people in this category, and they had neither S nor N antibodies detected in their blood. Except for one person. She was surprised to learn she of a silent previous infection based on the finding of both S and N antibodies in her blood. Subsequent testing of her husband, who also is unvaccinated without previously known infection, found S and N antibodies in his blood too, bringing the total number of people in this group to six with two outliers.
We can summarize what we’ve learned as follows:
- Both SARS-CoV-2 infection and vaccine stimulate the production of S-antibodies, 100% of the time in this study.
- A significant number of people, about 20% in this group, had silent SARS-CoV-2 infections during the pandemic.
- SARS-CoV-2 infection does not seem to stimulate the production of N-antibodies consistently. This is a pesky observation that does not fit our model.
Could it be that N-antibody production relates to the severity of disease? Probably not since quite a few of the S+ N+ individuals in this study had asymptomatic infections. Could it be that variant viruses cause N-antibody negative infections? Or is the N-antibody test not very good? All are possible, but, as we’ve said so many times since the outbreak of the pandemic, we really don’t know for sure. What we can say is that tests for “COVID antibodies” are more complicated than they seem at first glance. Laboratories should clearly label the antibodies measured when reporting SARS-CoV-2 antibody results.
How do the antibody levels caused by disease compare with the antibody levels caused by vaccine? And which vaccine provides the best immune response? We will examine these questions next time.
- A Useful Model
Scientists create mental models to help understand the world around us. Not that these models are reality; the real world is much, much more complicated. Instead, these models are useful ways to think about reality. Today I would like to create a mental model of the SARS-CoV-2 virus that will be useful as we learn more about the virus in coming weeks and months.
Think of the virus as an egg with spikes driven into the shell. Now focus on two parts of this model: the spikes and the yolk inside the egg. The spikes correspond to the S-proteins on the outside of the virus. That’s easy to remember—S for spike. The yolk corresponds to the nucleocapsid that covers the genetic material on the inside of the virus. Let’s call the nucleocapsid “N” for short, which will also help us remember that N-proteins are inside the virus. Now in our mind’s eye we see a virus shell with S-proteins on the outside and N-proteins on the inside.
When foreign proteins show up in your body, your immune system responds by making antibodies. Therefore, when infected by SARS-CoV-2, your body will make at least two different types of antibodies: S-antibodies and N-antibodies. Blood tests are now available that can detect both kinds of antibodies, and both should be detected in someone who has been infected by SARS-CoV-2 in the past.
Vaccines expose the body to S-proteins only. N-proteins are not part of vaccines. Therefore, someone who has received a vaccine but has never been infected will have S-antibodies but not N-antibodies. S-antibodies may come from vaccine or infection. N-antibodies come from infection only.
Now we can use our model to predict antibody test results from four different groups of people, represented in the table below:
Previously Infected Never Infected Vaccinated S+ N+ S+ N- Unvaccinated S+ N+ S- N- A simple model, but does it work? To find out, I collected the results of antibody tests from four groups of people: people infected but not vaccinated, people vaccinated but not infected, people vaccinated and infected, and people never infected nor vaccinated. Next time, we will review the results.
- New Clotting Disorder Caused by Vaccine
We’ve already discussed the rare clotting disorder associated with COVID-19 vaccinations, resulting in the pause of the Janssen vaccine last month. It’s time to take a deeper dive to understand more about this disorder. To start, we must learn a little about platelets. It’ll be quick, I promise.
Platelets are bits of cells that circulate in the blood stream looking for leaks. When a leak is found, platelets are activated and clump together to plug the hole. There are lots of platelets in blood, so one hole usually isn’t enough to reduce the platelet count. However, if all the platelets are activated at once, many clumps form, and the count of platelets goes down dramatically. The reduction of platelet count is called thrombocytopenia. “Thrombocytes” means “platelets” and “penia” means “not enough”, so “thrombocytopenia” simply means “not enough platelets”.
Heparin induced thrombocytopenia (HIT) is a condition in which platelets are activated after the use of heparin, causing a suddenly drop in platelet count. This is particularly dangerous because, as you may recognize, heparin is a “blood thinner” given to dissolve clots. The formation of many clots is the opposite of what is desired. HIT occurs because of an immune response in which antibodies to a molecule that forms when heparin is injected cause activation of platelets throughout the body. The molecule is called “heparin-platelet factor 4 complexes,” but the name doesn’t matter. Most people don’t have those antibodies to this molecule. This is a rare but life-threatening complication of heparin therapy.
The rare clotting disorders that have been rarely been observed after the Janssen vaccine have a similar mechanism. Now referred to as vaccine induced thrombotic thrombocytopenia (VITT), it is like HIT because antibodies develop after vaccine administration that cause platelet activation. The antibodies are similar enough to HIT antibodies that giving heparin will make the clots worse. This is why heparin cannot be used to break down those clots.
This seems to be the same clotting complication that has been observed with the AstraZeneca COVID-19 vaccine, not available in the U.S., but widely available elsewhere. Both vaccines have in common the use of an adenovirus vector to deliver the vaccine. A viral vector is not used in the mRNA vaccines. Is VITT related to the adenovirus vector in some vaccines? Nobody knows for sure. Yet.
This is another example of unintended consequences resulting from the use of systems still in the early stages of development. Life is full of risks; we accept that. But wisdom demands that risks be acknowledged, quantified, and mitigated as much as possible. Only the foolish follow science blindly.
- Why Vaccinate COVID-19 Survivors?
In these posts I use my experience as a practicing pathologist to present clear, simple, and understandable explanations of important issues relating to the pandemic amid the noise and misleading half-truths we encounter daily. When I don’t know, I tell you. Today, I’m asking you to help me understand something that’s been puzzling me for weeks. Why does the CDC adamantly insist that COVID-19 survivors be vaccinated?
The CDC’s statement is simple enough. They say that there is a wide range of outcomes to SARS-CoV-2 infection, from no effect to death, and that there is a corresponding range of immune responses to infection. Those who had mild disease, the argument goes, may not have built up the immunity necessary to fight future infections. The vaccine, on the other hand, is a measured dose designed to stimulate an adequate immune response. Furthermore, they assert that there is no data on how long natural immunity may last, saying, “experts do not yet know how long you are protected from getting sick again after recovering from COVID-19.” So, they conclude, everyone must be vaccinated, even those who have recovered from COVID-19.
Simple enough, yes. You will find this theory repeated on health websites and in the popular press, often citing compelling studies and medical experts.
But does it make sense? Before the pandemic, did medical science ever assert that vaccine-induced immunity is superior to natural immunity? I’ve looked. I cannot find that assertion from any reputable source, nor can I find that assertion supported by any body of evidence. I’m not saying that I’ve looked everywhere. I’m saying I looked and came up empty. If you know where it is, please tell me.
Let me be clear about my question. I’m not doubting that vaccine is an important tool in the war against infections generally and SARS-CoV-2 specifically. Clearly, vaccines provide protection to individuals most vulnerable to bad disease outcomes. Clearly, vaccines raise the overall immunity within the population, stemming the spread of infection. An article published in Texas Medicine on the eve of the pandemic advocates for vaccine, especially childhood vaccines—mumps, measles, rubella, and the like—using a simple risk-benefit analysis. This analysis, and many more like it within the body of traditional medical science, compare the risk of vaccine to the risk of disease. Acknowledging that vaccines have risk and diseases have risk, vaccines generally have less risk than disease. This is very different from introducing the risk of vaccine to individuals who have already survived the risks of infection by the virus.
There is a glaring flaw in the CDC’s argument. True enough, experts do not yet know how long you are protected from getting sick again after recovering from COVID-19. But neither do experts know how long you are protected from getting sick after completing a vaccine series. How could they know either? Neither COVID-19 nor the vaccines have existed long enough to be studied meaningfully, which brings me back to my question. How can we say vaccine-induced immunity is superior to natural immunity?
I cannot think of any other example of this line of thinking. We do not insist that children who have had chicken pox get the chicken pox vaccine. We do not give hepatitis B vaccine to individuals who have had hepatitis B infection. In fact, before giving a hepatitis B vaccine, we usually test for antibodies to make sure the individual has not been previously infected. Why expose someone to an additional risk unnecessarily?
Are COVID-19 vaccines different from any other vaccine? Has a new theory of immunology suddenly replaced years of observation and wisdom? Why would the CDC, a place I know to be filled with smart, dedicated, and sincere physicians and scientists, be so insistent that COVID-19 survivors be vaccinated?
If you know the answers, please tell me. I would love to hear from you.
- Herd Immunity
What is herd immunity and when will we get there?
Imagine a billiard table with balls racked at one end. Smash a cue ball into the neat arrangement and all the balls will move. That’s like the pandemic. The energy spread from ball to ball is like the spread of virus from person to person.
Now imagine the same table, except this time some of the balls are bolted onto the table so they can’t move. Smash a cue ball into the rack and not as many will move. The bolted balls are like people with immunity; they absorb energy and do not allow it to spread. How many balls must be bolted onto the table to prevent spread of motion across the table? That’s herd immunity; the percentage of people with COVID-19 immunity that it takes to stop the uncontrolled spread of virus.
Epidemiologists differ on herd immunity targets for COVID-19, with estimates varying from 60% to 90%. But these estimates are just educated guesses. Herd immunity is something observed, not something predicted. When the rates of disease reach a stable low level, herd immunity has been achieved.
Now some observations from my point of view. Last week, without a decline in the number of tests performed, there were only 6 positive SARS-CoV-2 tests in the laboratory where I work. Until last week, weekly positives have been in the double digits going back to April 2020, with a peak of 475 during the first week of this year. Since the last week in February, the weekly number of positive tests have been below 40. The curve has flattened, despite the lifting of many restrictions designed to prevent spread of the disease in Texas. We can no longer say that there is a COVID-19 epidemic in my community. Instead, the disease appears to have reached endemic levels here.
I need to pause to explain what I mean. Disease prevalence, which we’ve defined before, means the rate of disease in a population. Prevalence can be applied to any disease, not just infectious disease; thus, we can speak of the prevalence of diabetes, of breast cancer, of heart disease, and so on. Epidemic simply means increasing prevalence, just like acceleration means increasing speed. Endemic means that disease prevalence is stable and not changing. Epidemics can be local, meaning confined to a house or a neighborhood or a city or a country, or epidemics can be global, meaning happening all over the world at once. Global epidemics are called pandemics. The term “global pandemic” is as redundant as “unexpected surprise” or “advance warning.”
Herd immunity is achieved once an infectious disease reaches endemic levels, but what is that number? Assuming natural and vaccine-induced immunity are the same thing, then herd immunity is the percentage of folks who have either had the infection or the vaccine when disease becomes endemic. Today, it is estimated that 10% of Texans (2.8 out of 28 million) have had COVID-19, and that 35% of Texans have been fully vaccinated. Therefore, my area seems to have achieved COVID-19 herd immunity at 45%.
This all sounds like great news, so why not throw our masks in the air and celebrate? There are still unanswered questions. Vaccine-induced immunity is not the same as natural immunity, but is it the same enough for calculating herd immunity? How long does immunity last? Can herd immunity be lost once achieved? What will be the impact of emerging variants on immunity of individuals and populations? And, most puzzling to me, why is the virus surging now in India and Brazil despite previous waves of infection?
We still don’t know as much as we would like to believe.
- More Variants Emerge
As new variants emerge, it’s time to update our charts so you will know what’s coming and what to watch for. In its summary released last week, the CDC made minor terminology revisions and made some roster changes on the line-up cards. In this edition, we will highlight the changes and update our charts with the latest information.
Variants of High Consequence. Now called Variants of High Consequence instead of Variants of High Concern, these SARS-CoV-2 strains cannot be detected by tests, are not treatable by current therapies, or are not protected by natural or vaccine induced immunity. A strain that fits any of these categories must be reported to the WHO and CDC immediately. Thankfully, this list is still blank.
Variants of Concern. Variants of Concern have reduced detection by tests, reduced response to therapy, reduced immune protection, greater transmissibility, or more severe disease. Although there have been no additions to this list, there have been noteworthy updates to our understanding of these variants. For example, B.1.1.7, the UK Variant, and B.1.351, the South African Variant, remain at the top of the increased transmissibility list at 50%; however, as we predicted in January, B.1.1.7 is also now the most prevalent lineage of the virus in most regions of the U.S. except the west coast. The California Variants B.1.527 and B.1.529 are now considered the most resistant to therapy of all U.S. variants.
Variants of Interest. Variants of Interest are U.S. variants with the potential to become Variants of Concern based in the mutations within the variant, even though they don’t fulfill criteria to be a Variant of Concern based on observation. Two changes have occurred. First, B.1.525 is now believed to have first originated in the U.K. and Nigeria, even it continues to be most prevalent in New York. And second, since last writing, a new variant, B.1.526.1 has spun off the New York Variant B.1.526. This gives us the opportunity to briefly explain the classification system I have been using.
Because SARS-CoV-2 mutates so quickly, new variants emerge rapidly. The PANGO lineage system attempts to apply some order to this chaos. Names begin with a letter designating a unique lineage, followed by a series of numbers separated by dots. For example, the U.K. Variant B.1.1.7 is the seventh named variant of the B.1.1 lineage, and B.1.1 is the first named variant of the B.1 lineage, and so forth. By looking at the name B.1.526.1 we know that this variant evolved from the New York Variant B.1.526, but that it has enough unique characteristics to merit its own name. The variant’s family tree is embedded in the name. For example, B.1.1 and B.1.526 are siblings, B.1.526.1 and B.1.1.7 are cousins, and B.1 and P.1 are from totally different families. It’s a useful although not perfect system, and like everything in the pandemic, it continues to evolve.
Thousands of variants have been described. The ones highlighted in the charts below are currently considered the most important in the U.S:
- Janssen Pause
These blogs advocate caution and skepticism, specifically in response to the COVID pandemic, but more generally in response to all “scientific” proclamations. Don’t “follow the science” blindly. Instead use your “smell test” before believing anything labelled as science. Remember that science does not prove reality. Instead, science proves what is not real. We know much less than we would like to believe.
The sudden “pause” in vaccine rollout announced last week by Janssen is a case in point. The pause follows reports of six cases of unusual blood clots following administration of the vaccine, tragically including one death.
These unusual blood clots are called cerebral venous sinus thrombosis, or CVST, a condition which blocks the flow of blood out of the brain. As a result, the blood vessels may burst causing a stroke which may permanently damage brain tissue. So far, all patients are women under 50 years old with low platelet counts.
An association between COVID-19 and CVST was noted before the Janssen vaccine was released. In the August 2020 edition of the American Journal of Neuroradiology, Dr. D. D. Cavalcanti and associates reported three COVID-19 patients under 41 years old who developed CVST; all three patients died. Others have reported similar associations between CVST and SARS-CoV-2 infection.
This raises several questions. Can CVST be caused by COVID-19? Can CVST be caused by the Janssen vaccine? What about the mRNA vaccines? And how is it that a vaccine causes a complication of the disease it’s meant to prevent? Furthermore, six instances of CVST out of 6.8 million doses of the Janssen vaccine administered is a complication rate of less than 1 in 1,000,000. The rate of anaphylaxis associated with the mRNA vaccines is 10 times as high. Why so much concern for such a rare complication?
Something doesn’t smell right to me.
- Antibody Tests after Vaccination
The CDC recently updated guidelines for interpretation of SARS-CoV-2 antibody tests after infection and vaccination. There is currently no recommendation to measure antibodies after vaccination to determine vaccine effectiveness. Despite this, I know vaccinated individuals who measure antibodies anyway, and they are surprised when antibody tests come back negative.
Okay, full disclosure. It was me. And my wife. We took the Janssen vaccine in mid-March, and I checked our SARS CoV-2 IgG antibodies last week. They’re negative. For both of us. What’s going on here? Isn’t the point of vaccination to stimulate the production of antibodies?
The answer is a qualified yes. The qualification comes in two parts: the “scientific explanation” and my opinion.
First the “scientific explanation”, simplified. An individual may produce three types of antibodies against SARS-CoV-2: N, S or RBD. Infection stimulates the production of all three types of antibodies, but vaccine stimulates the production of S antibodies only. Therefore, vaccinated individuals who have never been infected will be S-antibody positive, but N and RBD antibody negative. If the antibody test is designed to detect N or RBD antibodies, but not S antibodies, then the result will be negative in those individuals. On the other hand, detection of N or RBD antibodies in a vaccinated individual means that the individual has been exposed to the virus, either before or after vaccination. The trouble is that the antibody tests available today by emergency authorizations do not specify which type of antibody is measured. We do not know which antibody we are measuring unless we know details about the test, details that are usually not listed on the report from the lab.
This explanation has precedent. We know, for example, that Hepatitis B infection stimulates the production of two different types of antibodies: core antibody and surface antibody. Hepatitis B vaccine only stimulates production of surface antibody; it does not stimulate production of core antibody. Therefore, someone who is positive for surface antibody only has been vaccinated but has not been infected. On the other hand, someone who is positive for both surface and core antibodies has been infected by Hepatitis B in the past.
All well and good for hepatitis, but what about SARS-CoV-2? In the case of SARS-CoV-2, the “scientific explanation” is a hypothesis, meaning it is an educated guess. Before we can say that we know something, we must compare our hypothesis to real-world observations. There has not been enough time to observe the response that our bodies really have to vaccine. It doesn’t make the hypothesis wrong, but it doesn’t make it right either.
My opinion? The “scientific explanation” is still an opinion.
- Anaphylaxis
In the revised EUA issued for its COVID vaccine on February 25, 2021, the FDA required Pfizer to updated its “Fact Sheet for Healthcare Providers” to include post-authorization adverse effects. As a result, Pfizer’s fact sheet now states, “Severe allergic reactions, including anaphylaxis [emphasis added], and other hypersensitivity reactions (e.g., rash, pruritus, urticaria, angioedema) have been reported following administration of the Pfizer-BioNTech COVID-19 Vaccine during mass vaccination outside of clinical trials.” Moderna did not receive the same mandate to revise its fact sheet, which still does not include a similar warning about anaphylaxis. What is anaphylaxis and what are the facts about this life-threatening vaccination complication?
Anaphylaxis is a severe allergic reaction in which your body releases a flood of chemicals designed to modulate the immune response all at once. The result is a sudden drop in blood pressure and narrowing of airways which can lead to fainting and death. Some people are more prone to anaphylaxis than others, and some stimuli are more common causes of anaphylaxis than others. Peanuts and bee stings are common examples. The allergic response can be effectively reversed by an injection of epinephrine. Susceptible individuals (and you know who you are) often carry EpiPens to self-administer a dose of epinephrine in case of a reaction.
Anaphylaxis can occur anytime something is injected in the body, although the risk is exceedingly low. However, the rate of anaphylaxis after the mRNA vaccines is about ten times higher than the rate of pre-COVID vaccines. If this is the case, then why did Pfizer’s new EUA highlight this potential complication and Moderna’s did not? The answer may be related to initial experience with the two vaccines. Since Pfizer received authorization for its vaccine first, increased anaphylaxishad already been observed in association with the Pfizer vaccine before Moderna even received its EUA. The reputation stuck. Although initial reports suggested that Pfizer caused more than twice as many anaphylaxis reactions as Moderna, subsequent experience has shown that both mRNA vaccines have about the same rate of anaphylaxis. According to a March 16 CDC report 1,913 deaths have been reported associated with vaccine administration after more than 109 million doses. Reports of recent VAERS data searches, the FDA database collecting vaccine adverse events, suggest that the rate of anaphylaxis deaths are similar for the two vaccine manufacturers. The Janssen recombinant vector vaccine appears to be associated with fewer cases of anaphylaxis than the mRNA vaccines; time will tell whether this observation sticks or is skewed by the fewer number of vaccines administered so far. The CDC recommends that all vaccination administration sites be prepared for potential anaphylaxis reactions, including educating staff on the signs and symptoms of anaphylaxis and having at least three epinephrine doses on hand at all times.
A few sensible conclusions may be drawn from this information.
- Ask the person administering your vaccine what would happen if you had an anaphylaxis response.
- If you have an EpiPen, bring it with you when you get your vaccine.
- If you have had a severe allergic reaction in the past, consider deferring vaccination or taking the Janssen (Johnson and Johnson) vaccine instead of an mRNA vaccine.
- Breakthrough
As more Americans are receiving COVID vaccinations, there are reports of COVID occurring in individuals who have been fully vaccinated. Can this really happen?
Yes, you may still become sick from a SARS-CoV-2 infection even if more than two weeks have passed since your final vaccine injection. “Breakthrough” is the term for this type of infection, and many state health departments have reported breakthrough infections. According to current CDC reports, over 50 million Americans have been fully vaccinated, accounting for 15.1% of the total U.S. population, yet 7-day rolling averages for new COVID-19 cases and hospital admissions for COVID are up 6.7% and 2.6% respectively.
We know that breakthrough infections occur with other vaccines. In years past, many patients were admitted to the hospital for flu even though they received a flu vaccine earlier in the season. We may be seeing a similar phenomenon with the COVID vaccine. Furthermore, we still do not know whether most breakthrough infections are caused by the original SARS-CoV-2 virus, or one of the emerging variants. It is possible that vaccine is less effective against one or more variants.
We have a lot to learn about breakthrough infections, but this much is clear: the pandemic is not over, and the vaccine is not a panacea. While vaccine may provide an added layer of protection against dying from COVID, it does not prevent contraction of disease. For now we must continue to do what we know keeps us safe: mask in public and keep apart, even if you have received a vaccine.
- New Variant Classification
Last week the CDC revised its classifying terminology for SARS-CoV-2 variants. To have clarity in our thoughts and debates, we must be precise in our language. Poor decisions often descend from muddled and incomplete understandings. I know that readers of these posts strive to be current in models of understanding and language, so they will not be caught flatfooted in conversation and reasoning. That’s why I summarize the essential points here.
There are now three types of SARS-CoV-2 variants: Variants of Interest, Variants of Concern and Variants of High Concern. I will discuss the definitions, lists of variants and their characteristics in reverse order.
Variants of High Concern. Variants of high concern are those SARS-CoV-2 variants that cannot be detected by tests, are not treatable by current therapies or for which natural or vaccine induced immunity offers no protection. Any one of those three criteria is enough to place the variant on the High Concern list. Scary stuff. The good news is that there are no variants on this list. At least not yet.
Variants of Concern. Variants of Concern have reduced detection by tests, reduced response to therapy, reduced immune protection, greater transmissibility, or more severe disease. Again, any one of these criteria is enough to land a variant on this list. The bad news is that the number of variants on this list has exploded since the last time I wrote about it. In addition to the B.1.1.7 variant first detected in the UK last fall, four other variants have been added to the list:

These Variants of Concern have all been identified in the United States. The B.1.427/429 Variants of Concern are most prevalent in the western United States, now responsible for more than half of infections in California. The B.1.1.7 Variant of Concern is most prevalent in New Jersey and Florida, approaching 10% of the new viral infections there. Click here to view the current numbers and distribution in the United States. To see worldwide cases of COVID-19 caused by variants, click here. These maps are updated at least weekly.
Variants of Interest. Variants of Interest are being watched closely because they have the potential to become Variants of Concern based in the mutations within the variant, even though they don’t fulfill criteria to be a Variant of Concern based on observation. This may be because the variant is too new or because too few of the instances of the variant exists to make meaningful observations. The current Variants of Interest and their potential, but not observed, effects are listed below:

Like the Variants of Concern, all the Variants of Interest are currently present in the United States.
There are a number of other variants which have been identified and named, but which have not yet been classified as a Variant of Interest, Variant of Concern, or Variant of High Concern. Expect the members of these variant classification lists to change and shift as more becomes known about variants.
- New Guidance for the Fully Vaccinated
Yesterday, the CDC published new guidance for fully vaccinated individuals. In this article, we will summarize the key points of this new guidance.
First, we must understand what it means to be fully vaccinated. The full effect of vaccine-induced immunity takes about 2 weeks, so an individual is considered fully vaccinated 14 days after the final vaccine injection. The final vaccine injection is the second dose of the Pfizer or Moderna vaccine, or the single dose of the Janssen vaccine.
Last month, the CDC issued guidance lifting the quarantine requirements for fully vaccinated individuals following a COVID exposure, provided they remain asymptomatic. Previously, this permission expired after 90 days. Yesterday, the CDC affirmed its previous guidance, but lifted the 90-day expiration. According to current CDC guidance, there is no longer an outer time-limit for the benefit of vaccine-induced immunity. This is bound to change; we will follow closely.
To the removal of quarantine requirement, the CDC also added two additional liberties yesterday: (1) fully vaccinated individuals may visit indoors with other fully vaccinated individuals without wearing masks or social distancing, and (2) fully vaccinated individuals may visit with unvaccinated people from a single household who are at low risk for COVID-19 without wearing masks or social distancing.
Other COVID precautions remain in force for fully vaccinated individuals, including masking and social distancing in public except in the specific situations mentioned above. If symptoms develop, fully vaccinated individuals should follow the same quarantine and testing recommendations of unvaccinated individuals.
- New Vaccine
There were a couple of big changes in the COVID vaccine landscape last week. On Thursday, February 25, the FDA reissued its EUAs for the Pfizer and Moderna COVID-19 vaccines, revising portions of their original EUAs. On Saturday, February 27, the FDA issued a new EUA for the Janssen COVID-19 vaccine, commonly known as the Johnson and Johnson vaccine. Lots of news, too much for one blog. Let’s address the important information one bite at a time, starting with the Janssen vaccine.
Like all other COVID-19 vaccines, the Janssen vaccine has not been approved for use by the FDA. Instead, these vaccines are authorized for use in the U.S. This authorization is based on the FDA’s authority to make unapproved products available during an emergency when “there are no adequate, approved, and available alternatives.” As stated in the EUA letter issued February 27, 2021, “It is an investigational vaccine not licensed for any indication.” This means that clinical trails on vaccine safety and effectiveness have not been completed. Expect comprehensive analysis of clinical trials this summer at the earliest.
However, the Janssen vaccine differs from the other two vaccines in important ways. First, it is not an mRNA vaccine. Rather, it is a recombinant vector vaccine. This vaccine is made by inserting genetic code for a protein of the target into a harmless virus (the “vector”). When injected, this harmless virus presents the target proteins to the immune system, causing formation of antibodies, in this case antibodies to the spike proteins on the SARS-CoV-2 capsule. This technology is not entirely new. Manufactured (or “recombinant”) genetic code has been used to synthesize proteins for vaccines for nearly a decade. Recombinant flu vaccines received FDA approval in 2013. You may have received a recombinant flu vaccine in recent years. The difference between recombinant protein vaccine and viral vector vaccines has to do with where the antigenic proteins are made–either in your body (viral vector) or outside your body (recombinant protein). The harmless virus (the “viral vector”) cannot replicate within your body, so the effect is the same.
There are more differences. According to data submitted to the FDA, the Janssen vaccine is less effective preventing moderate to severe COVID-19 than the Moderna and Pfizer vaccines. The Janssen vaccine requires only one doses compared to the two doses required by Moderna and Pfizer. Storage of the Janssen vaccine is easier to accomplish than the other two. Vaccines features are compared as follows:
Pfizer Moderna Janssen Vaccine Technology mRNA mRNA Recombinant Vector FDA Approval No No No Effective rate 95% 95% 66% Minimum Age 16 years 18 years 18 years Doses 2 2 1 Storage -70°C -70°C Refrigerated Time between doses 3 weeks 1 month Not applicable Current comparison among authorized COVID-19 vaccines. There is another difference. In its reissued EUA, the FDA has required Pfizer to disclose post-authorization adverse events in its fact sheet to health care providers. We will discuss that next time.
- Vaccine and Quarantine
On February 10, the CDC updated quarantine guidance for vaccinated individuals exposed to COVID-19, giving some people a get out of jail free card.

According to the new guidance, individuals who received their second FDA authorized mRNA vaccine injection between 14 and 90 days ago need not quarantine after exposure to COVID-19 provided they are symptom free.
An exposure is still defined as an encounter of more than 15 minutes and less than 6 feet with someone infected by SARS-CoV-2 when one or both individuals are not wearing a mask. Provided that there is no fever or other indications of upper respiratory infection in the exposed individual, quarantine is not necessary for those who received both doses of either the Pfizer or Moderna vaccine more than two weeks before the exposure. However, vaccinated individuals should monitor for symptoms (i.e., take daily temperatures) for 14 days after exposure, and should quarantine immediately if symptoms (i.e., fever) develop. This reduced quarantine requirement does not apply to individuals who complete a vaccination series which has not receive an EUA from the FDA, such as vaccines approved in countries outside the United States.
If it has been more than two weeks since you completed a vaccine series, then you benefit from reduced quarantine requirements after exposure. But you don’t get to party like it’s 2019! You may still be able to spread the virus to others, so you must still mask and social distance in public. Furthermore, no one knows how long vaccine-induced immunity will last.
The CDC maintains that natural immunity—immunity from infection—lasts for at least 90 days. It may last longer, but the CDC is still unwilling to say so. Since the CDC’s new quarantine exemption also expires after 90 days, it seems reasonable to infer that 90 days may be the outer limits of immunity, whether from previous infection or vaccination. We may hope that it’s longer, but so far, the CDC has not said so.
So what does all this mean? If it has been more than two weeks since you completed Pfizer or Moderna vaccination series, you have a get out of quarantine jail free card—you don’t have to quarantine after a potential exposure if you are symptom free. However, a vaccination does not make you special in any other way. You must monitor for symptoms for 14 days after exposure. You must quarantine immediately if you have symptoms. You must continue to mask and keep apart in public. In other words, even if you have completed a vaccination series, you don’t have this card:

At least not yet.
- Shouldna Taken That Shot
It was a heady time to be a scientist. Albert Einstein was still alive, and his special and general theories of relativity changed our understanding of the universe. Quantum physics predicted space travel and limitless energy. We had a brand-new theory of gravity, of space-time, of waves and particles, and of the atom. Vaccines had nearly wiped smallpox off the earth. We had penicillin, saving many lives and limbs. Science, it seemed, could conquer all. So, when your doctor said you needed a shot to prevent a miscarriage, you took an injection without question.
DES (diethylstilbestrol) is a synthetic estrogen created by Sir Charles Dodd in 1938. Cheap and easy to produce, pharmaceutical companies marketed DES for prevention of menopause symptoms in women. In 1947, the FDA approved DES for use to prevent miscarriages, and such use was advocated by an article published in the American Journal of Obstetrics and Gynecology. American obstetricians enthusiastically embraced the new drug as a cure for one of the most unhappy outcomes in their profession. Although some physicians questioned its effectiveness, DES continued to be commonly prescribed in the United States to women with threatened miscarriages until 1971.
That’s when a bombshell was published in the New England Journal of Medicine. The daughters of women who received DES during pregnancy had an unignorably high rate of clear cell adenocarcinoma of the vagina, an extremely rare tumor in women whose mothers had not received DES. That’s right—a drug manufactured and sold in the United States, approved by the FDA, prescribed as intended by licensed physicians—caused a rare cancer in young women. And not just clear cell adenocarcinoma. The daughters of women who received DES during pregnancy have higher rates of breast cancer, abnormal cells on their pap smears, anatomic defects in their reproductive organs, trouble getting pregnant, and problems during pregnancy. And not just the daughters—the sons too have increased rates of benign tumors and structural defects in their reproductive organs. Even the mothers are affected. Women who received DES during pregnancy have an increased risk of breast cancer. Does it stop there? Research is currently ongoing on the third generation, the grandchildren of women who received DES during pregnancy.

Clear cell adenocarcinoma of the vagina. Although it’s not a story my profession likes to tell, the lessons of the DES tragedy must never be lost. Before we accept the opinions of experts, we must be mindful of the limitations of science. Before we are swept along with the crowd, we must recognize the possibility of unintended consequences. Before we act on conventional wisdom, we must think; think with our own brains, and make up our own minds. We must ask questions, critically examine data, and make judgements by what we know from experience. We must all be scientists now.
- We Have No Bananas
When Texas freezes over, most everything closes. That includes blood collection centers, which were closed for 5 days this week. I’m writing to encourage you to donate blood. If you’re a bottom-line person, you can skip this blog, find a donation site, and sign-up to give blood by clicking here.
For those of you still with me, this is what I saw at the grocery store last night:

There were no bananas. What does that have to do with blood donation? Read on; I’ll tell you.
Blood has four parts. First, there are the red cells which carry oxygen to the tissues in your body. Oxygen is the fuel that makes cells go. Without oxygen, cells get cold and die. When people bleed, they lose these fuel-carriers, and their body goes on the biologic version of rolling blackouts, shunting blood towards essential internal organs at the expense of less vital parts like fingers and toes. The second part of blood are white cells. These are the infection fighting cells of your immune system. Like first responders, white cells are carried by blood to the front lines of battle, where they protect you from invasion. Third, blood contains platelets which are little bits of larger cells that act like the Fix-A-Flat you put in bicycle tires. Platelets circulate in the blood looking for holes to plug, helping slow down or stop bleeding. The fourth part of blood is plasma, the liquid part. Plasma contains proteins, hormones, antibodies, clotting factors, and all the other stuff that needs to be carried from one part of your body to another.
Most people have all four parts of blood in excess, but the blood center will test before collection to make sure you will not miss the unit you donate. The unit you give is divided into three parts, so every donation helps three different people. The collected red cells are separated into one bag, the platelets into another bag, and the plasma into a third bag. The white cells collected are not used.
Red cells are like milk. They must be refrigerated, and they expire after about a month (up to 42 days). Plasma is like frozen vegetables. Once frozen, plasma can be stored for a year. But platelets are like bananas. They are stored at room temperature, and they are only good for five days. So when Texas freezes over, we run out of bananas, and we run out of platelets.
Blood bank inventories are slim during the first part of the year. After the holidays, people don’t feel like donating blood. That’s understandable, but our hospital blood banks suffer critical shortages as a result. This year is no exception; blood banks were dealing with critical shortages before the freezing weather. But two massive winter storms this week have reduced blood inventories to nearly nothing. That’s why your urgent action is needed.
There is no substitute for donated blood. There are no synthetic red cells or platelets, and there is no substitute for human plasma when it is needed. To have blood products available when you or your family need it, you must make blood available to your neighbors today. Please, your community needs your blood. Find a donation site, and sign-up to give blood by clicking here.
- mRNA Vaccines
To understand how mRNA vaccines work, we must first have a basic understanding of cells and genetics. Zzzzzzz. Wait! Before you go to sleep, we’re going to make this really short and really simple. Cells are bags of jelly—jellybeans, so to speak—and in those jellybeans is a kernel called a nucleus. DNA lives in the nucleus, and like the cell’s hard drive, DNA stores and preserves the cell’s genetic code. Genetic code is a series of nitrogen bases strung together to form nucleic acid. There are only four possible bases, so just like computer code is a series of 1’s and 0’s, genetic code is a series of A’s, T’s, G’s, and C’s, each letter standing for a different nitrogen base. DNA is arranged in two complimentary stands—the famous double helix of Watson and Crick—to create code redundancy like mirrored hard drives that protect your data in case of a crash.
When the genetic code needs to be accessed, a specific portion of the DNA untwists, exposing a segment of code which is copied onto a new strand of messenger RNA (mRNA). Unlike DNA, RNA is only a single strand of nucleic acid and much less stable. The mRNA floats into the cell jelly, the cytoplasm, where ribosomes attach and move along the strand, coupling together amino acids as they go. Every sequence of three bases on the mRNA, known as a codon, codes for a specific amino acid. For example, GCA codes for alanine, CAA codes for glutamine, and so on. There are 20 different amino acids, each with its own codon or codons (some have more than one). Put together according to the sequence of bases on the mRNA, the amino acid chains become a protein. Out of the trillions of possible amino acid combinations, the proteins formed by your genetic code define the shape of your nose, the length of your bones, the complexion of your skin and everything else that makes you you. Once the right number of proteins have been made, the mRNA disintegrates into the cytoplasm of the cell. The process starts again in the nucleus, and a new protein is created as called for by the cell.
What if mRNA could be injected directly into cytoplasm without first being created in the nucleus? Then the cell’s machinery could create a protein that wasn’t part of the cell’s genetic code. That’s exactly the hypothesis behind mRNA vaccines. After the vaccine delivers mRNA into the cytoplasm of muscle cells in the arm, those cells begin forming the protein coded by the mRNA in the vaccine—in the case of COVID vaccines, one of the spike proteins known to exist on the SARS-CoV-2 viral capsule—and those proteins make their way to the surface of the cell where the immune system forms antibodies which are memorized by the body for future use. How cool is that!
Various companies have been working on mRNA vaccines for over a decade, but none made it to production until the pandemic demanded rapid vaccine development. Although never been used on a large scale before, mRNA vaccine technology is appealing for several reasons:
- Molecular sequencing systems makes creation of mRNA almost as easy as writing a computer script.
- Once sequenced, mRNA can be mass produced easily and cheaply.
- There is no danger from viable pathogens in the vaccine production.
- There are no infectious agents or toxins injected into the vaccine recipient.
- Once the delivery system is perfected, vaccinations for many different pathogens can be created by simply altering the mRNA sequence, making it possible for vaccines to respond quickly to emerging viral variants.
Before we anoint mRNA vaccines as our pandemic savior, we should first listen to voices urging caution about this new technology. For example, in a recent New England Journal of Medicine publication, Dr. Mariana Castells and Dr. Elizabeth Phillips note that the incidence of anaphylaxis, a serious, sometimes fatal allergic reaction, associated with the Pfizer SARS-CoV-2 mRNA vaccine is “10 times as high as the incidence reported with all previous vaccines, at approximately 1 in 100,000, as compared 1 in 1,000,000.” Why? And moreover, what are our expectations of vaccination? Do vaccines prevent COVID or simply reduce COVID complications? How long will immunity last? Who should NOT get the vaccine? Answers to these and other questions are not readily apparent, not because of a failure of diligence, but because there has simply not been enough time to collect, compile and analyze the data that will eventually yield answers.
The Center for Evidence Based Practice at the University of Pennsylvania recently published a review of the adverse effects of mRNA vaccines. Among their findings are the following:
- There are no specific guidelines for use of messenger RNA (mRNA) vaccines or contraindications to mRNA vaccines.
- No large trials of any mRNA vaccine have been completed yet.
- The only evidence on safety of mRNA vaccines comes from small phase I and phase II trials of SARS-CoV-2 vaccines, with follow-up typically less than two months.
- Systemic adverse events such as fatigue, muscle aches, headache, and chills are common
- The rate and severity of adverse events appears to be higher for the second dose of vaccine than for the first.
- Higher vaccine doses appear to increase the rate and severity of adverse events.
- Larger trials of SARS-CoV-2 vaccines are in progress, with results expected in mid-2021.
- There is not sufficient evidence to support any conclusions on the comparative safety of different mRNA vaccines.
- Direct evidence on the comparative safety of mRNA vaccines and other vaccines is lacking.
Clearly, mRNA vaccines offer an attractive, promising alternative to other vaccine technology, especially when a new vaccine is needed quickly. However, it is a new technology associated with risks of the unknown. Many unanswered questions remain, demanding a sober examination of the evidence for and against vaccine safety. Since the risk-to-benefit ratio from taking a COVID vaccine varies individually, I urge individual decisions, not collective ones. The Infectious Diseases Society of America recently published a comprehensive FAQ on vaccine safety which you may find to be a valuable great resource for making an individual decision.
Although paved with good intentions, the early path of new technologies is frequently littered with unintended consequences. Next time, I will tell a story of good intentions that ended tragically for many.
- The Latest about Variants
The CDC recently released new information about the variants of SARS-CoV-2, updating information previously released.
Although SARS-CoV-2 mutates frequently, about once every two weeks, most mutations do not result in a clinically different virus. However, three variants have emerged which are being watched closely.
B.1.1.7 is the first variant of concern which emerged in the UK last December and is now present in at least 70 countries, including the United States. This variant is associated with a fifty percent higher transmission rate, which means it may soon be the dominant form of the virus. There is emerging data that suggests this form of the virus is also associated with a higher death rate.
B.1.351 emerged in South Africa and has spread to other countries, including the United States. There is data that suggests that the Moderna mRNA-1273 vaccine currently used in the US may be less effective against this variant.
P.1 has been found in Japan and Brazil. As of late January, this variant is known to exist in the United States. There is data suggesting this variant may be less susceptible to immunity acquired either by previous infection or by vaccination.
All three variants are concerning because of mutations in the spike proteins in the virus. These proteins are significant because they are responsible for the binding of virus to cells in the back of the nose, the first step in infection. They are also significant because antibodies in the human immune system work by recognizing these spike proteins. Whether these antibodies come from natural immunity (i.e., previous infection), induced immunity (i.e., vaccination) or convalescent plasma, altered spike proteins may allow viral particles to slip past this line of protection.
Since we’ve talked a lot about vaccination recently, now may be the time to discuss how COVID vaccines work. We will pick up there next time.
- The Mask Clinic
Face coverings, N95 masks, respirators, and P99 masks—how do we make sense of this confusing alphabet soup?
Standard face coverings do not have a rating. They made from cloth or paper, and they usually resist fluids. But they leak. Air comes in around the sides–anyone who has worn a mask (and who hasn’t?) knows this. Nevertheless, mask usage is key to protecting you from exposure to SARS-CoV-2, the virus that causes COVID-19. However, there are more infectious organisms that require a rated mask for protection. One such organism is Mycobacterium tuberculosis, the organism that causes tuberculosis. Another such organisms may be the B.1.1.7 variant of SARS-CoV-2, the variant of concern, which has a transmission rate fifty percent greater than standard SARS-CoV-2.
Rated masks have a letter prefix, either N, R, or P, followed by a number, usually 95, 99 or 100. The letter refers to how resistant the mask is to oil, and the number refers to the percentage of airborne particles filtered by the mask.
Mask Type Airborne Particles Filtered Resistance to Oil N95 At least 95% No N99 At least 99% No N100 At least 99.97% No R95 At least 95% Somewhat P95 At least 95% Strong P99 At least 99% Strong P100 At least 99.97% Strong These masks are held snuggly around the face by elastic bands or straps around the head that eliminate the gaps between the skin and the mask. Note that “KN95” masks do not meet U.S. standards, and often have bands that loop over the ears and not over the head. Don’t let the word “respirator” confuse you: respirator is just another name for a rated mask. All the masks in the table above are also known as respirators. For protection against most respiratory organisms, an “N” mask is adequate since resistance to oil is not necessary.
So what level of protection is needed? Standard face coverings are adequate protection against SARS-CoV-2 exposure if worn properly by all individuals interacting at distances less than six feet, but an N95 mask is needed to provide adequate respiratory protection against tuberculosis. At 2 microns long, tuberculosis organisms are much larger than SARS-CoV-2 particles which measure 0.1 microns or less. Still, I believe that N95 masks also provide adequate protection against COVID, even when unmasked, infected individuals are nearby because of the experience of collectors at the test collection centers run by the laboratories where I work. These collectors use an N95 mask and a face shield for respiratory protection, and none has become infected at work despite collecting thousands of positive swabs.
How does an N95 mask work? In addition to forming a tight seal on the face around mouth and nose, N95 masks are made from material with pore sizes between 0.1 and 0.3 microns in diameter.
“But wait!” you might say, “You said that a SARS-CoV-2 virus particle is 0.1 microns or less. What keeps the virus from slipping through?” The spread of SARS-CoV-2 virus is on respiratory droplets. These droplets are 5-10 microns in diameter, much larger than the pore size of the masks, keeping most viral particles out of the nose of the mask wearer.
What about the coming B.1.1.7 variant of SARS-CoV-2? I want to be very clear: the FDA does not recommend the general use of an N95 or higher rated mask for COVID-19 prevention. Although N95 masks protect against SARS-CoV-2, there continues to be supply shortages of these masks. Therefore, the FDA recommends that their use be reserved for health care providers. However, as we discussed last time, there may soon be a time that this recommendation changes. It is possible that an N95 mask will be required to protect against the B.1.1.7 variant because of its higher transmission rate.
So what other new information is there about the SARS-CoV-2 variants? We will discuss the latest information about variants next time.
- Where’s the Flu?
Since October, all rapid SARS-CoV-2 PCR tests performed at the hospital laboratories where I work have included a PCR test for flu. But of the thousands of tests performed, not one positive flu has been detected. Has COVID cured flu?
No, I don’t believe that COVID has cured the flu, but I believe that masks have dramatically reduced the prevalence of flu in the community. Flu is a respiratory infection, passed from person to person by the same transmission mode as COVID, mainly inhaled droplets from an infected person. Standard face coverings reduce flu transmission in two ways. First, droplets from an infected person are less likely to be spread into the surrounding air; instead, they hit the mask and fall. Second, the mask helps filter the air of droplets that may contain viral particles. The result is a reduction, but not an elimination, of respiratory viral transmission.
So why haven’t masks cured COVID? SARS-CoV-2 is more infectious than flu, meaning that compared to flu, far fewer SARS-CoV-2 viral particles are needed to cause infection. Masks reduce the number of viral particles in the air, but they don’t eliminate them. Some virus leaks out from the masks of infected persons, and some virus can be inhaled by masked individuals nearby. It’s a matter of how much virus gets inhaled. It takes much more flu to cause infection than SARS-CoV-2. Masks slow the spread of COVID-19, but do not eliminate disease the way masks have flu.
We may use this COVID/Flu comparison to make some predictions about the B.1.1.7 variant, the “variant of concern” now reported in at least 70 countries. This variant is reported to be much more infectious than the standard SARS-CoV-2 virus, about fifty percent more, with the consequence that masks may not be enough to slow its spread through the community. Tighter, less permeable, and more uncomfortable masks may be necessary to protect against this variant as it spreads across our nation. The higher transmission rate also predicts that this variant will soon be the dominant form of the SARS-CoV-2 virus in the U.S.
If standard face coverings may soon become less effective protection against COVID-19, maybe now is the time to learn about different types of masks. We will do that next time.
- New Information about Variants and Tests
On January 8, the FDA released a warning that certain PCR tests for SARS-CoV-2 available by EUA may have seriously reduced sensitivity for the SARS-CoV-2 Variant of Concern (VOC, also known as 20I/501Y.V1, VOC 202012/01, or B.1.1.7), resulting in false negative test results. The tests mentioned in this advisory are the Accula SARS-Cov-2 Test by Mesa Biotech, the TaqPath COVID-19 Combo Kit by Thermo Fisher Scientific, and the Linea COVID-19 Assay Kit by Applied DNA Sciences. How will this development impact testing?
The SARS-CoV-2 virus mutates regularly with new strains emerging once every two weeks. Mutations occur in the genetic material of the virus, the very material that molecular test methods like PCR use to detect the virus. Until recently, none of these mutations has been associated with different clinical characteristics, such as more severe disease or increased rate of transmission. However, a variant of concern (VOC) recently emerged in the UK. As far as we know, this is still the one and only VOC. Since this VOC has a much higher rate of infectivity than standard SARS-CoV-2 virus, we can expect it to spread quickly. It will probably soon become the predominant form of the virus in the United States.
PCR tests look for a match in a region of viral RNA. The target sequence is like a computer password: any mistake causes the password to fail, even if the entry is off by only one letter. Therefore, when a mutation occurs in the target region of a PCR test, the test will be unable to detect the virus. This is why the tests mentioned in the FDA warning may not detect all forms of the virus.
Most PCR tests look for a match in more than one target sequence of RNA. Generally, the more targets in a particular test system, the less likely a mutation will impact test results. But beware: negative results should be evaluated in combination with history and symptoms. If COVID-19 is still suspected after a negative test, consider repeat testing with a different test—one with different targets.
How do you know which test you received? Look closely in the fine print of the results—the test used is probably referenced there. If not, ask.
Although most commercially available tests will continue to detect the VOC, these tests do not identify whether the virus is the variant or standard form. They will only identify that a SARS-CoV-2 virus is present. Furthermore, there is no assurance that a variant will not emerge that evades detection.
Obviously, this is a situation we will continue to follow closely.
- The FDA and Its EUAs
We have learned that science is a method, not a product. Science begins with an educated guess which is proven true by a series of experiments designed to show that the guess is false. If the hypothesis cannot be proven false, it is accepted as true by the community of scientists. Now that we’ve waded up to our armpits in philosophy of science, let’s move back into shallow waters and consider the process by which our FDA approves new drugs, medical devices, and laboratory tests in the United States.
First, I am going to reveal a personal bias. I believe that the United States has the safest healthcare system in the world for individual patients. Notice I did not say most efficient, cost effective, or optimized for populations. But if I am sick or injured, I want my healthcare delivered by U.S. trained doctors in U.S. hospitals using drugs, devices and tests approved by the U.S. FDA.
The FDA has been disparaged for being too slow to approve new therapies and methods. True enough, the FDA’s priority is not speed. Instead, the FDA’s mandate is safety. The FDA conducts a thorough, time-consuming review of all details of science supporting an application for approval, granting approval only after all questions have been answered satisfactorily. The FDA conducts post-market surveillance of approved drugs, devices and tests, mandating reporting of adverse outcomes. The FDA’s slow, methodical pace keeps Americans safe.
The FDA does not conduct science. Rather, the FDA performs quality control for science, validating the logic, analytics and data supporting the claims of products submitted for approval. Therefore, FDA approval implies a level of trustworthiness akin to science. But like science, FDA approval takes time. Time is something we do not have in a pandemic.
Enter the Emergency Use Authorization, known as EUA. When time is short, the FDA may allow unapproved medical products to be used to diagnose, treat, or prevent serious or life-threatening diseases or conditions when there are no adequate, approved, and available alternatives. All SARS-CoV-2 tests have been made available by EUA. Convalescent plasma is transfused under EUA. Antibody treatments for COVID-19 are prescribed under EUA. Remdesivir, Baricitinib and the their combination are first line treatments for severe COVID-19, available for use by EUA. And COVID-19 vaccines released by Pfizer and Moderna have been made available by EUA. None have been approved by the FDA. The trust conferred by FDA approval should not be transferred to the tests, treatments, or vaccines we are using in the fight against COVID-19.
Are there reasons to believe that the vaccines are safe and effective? Yes, and good ones too. But as with any experimental treatment or product, risks of adverse outcomes are elevated. Individuals must evaluate whether the risks–both known and unknown–are outweighed by the potential benefits of the vaccine. In a recent article published in the New England Journal of Medicine, Dr. Mariana Castells and Dr. Elizabeth Phillips articulately summarize the outstanding questions about the vaccines currently available:
“In the world of Covid-19 and vaccines, many questions remain. What are the correlates of protective immunity after natural infection or vaccination? How long will immunity last? Will widespread immunity limit the spread of the virus in the population? Which component of the vaccine is responsible for allergic reactions? Are some vaccines less likely than others to cause IgE- and non-IgE–mediated reactions? Careful vaccine-safety surveillance over time, paired with elucidation of mechanisms of adverse events across different SARS-CoV-2 vaccine platforms, will be needed to inform a strategic and systematic approach to vaccine safety.”
Some may criticize me for suggesting that the vaccine is not risk-free and that it may be better for some to wait before receiving their shot. However, honesty is one of the foundational characteristics of science. We must be willing to follow the data where it leads, even if it leads to a place we do not want to go. It is dishonest to say that any COVID-19 vaccine has FDA approval; to say that possible adverse effects—short term and long term–have been fully evaluated by the scientific method; to say that the protective immunity imparted by vaccine has been fully studied scientifically; to say that vaccine will alter the course of the pandemic or any infected person’s disease. I am not saying the vaccines will cause harm, but likewise we cannot say the vaccines will not cause harm.
The vaccines available now are associated with the risks of the unknown. For some that risk is worth taking; for others it is not. Whether you decide to take the vaccine or to wait, keep doing what we know slows the spread of disease: mask up, keep apart, and isolate when exposed.
- The Science of COVID
Spoiler alert: This essay contains an unpopular conclusion, and you may disagree. It’s okay if you do, because you’ll probably be in the company of many of my colleagues who disagree with me too. Today I’m going to talk about when we can trust science. To do that, I’m going to pretend to be a scientist and a philosopher. This is dangerous because, as I have said before, I am neither a scientist nor a philosopher. Instead, I am a practitioner, applying science to the problems of diagnostic medicine. As a practitioner, I must know when science is applicable and when it is not. I know just enough about science and philosophy to be dangerous.
Our experience tells us to trust science, and the explosion of technology during our lifetimes tells us we can. But science is a process, not a product. Not everything labelled as science is science. To understand the difference, let’s consider how science works.
The scientific method begins with a hypothesis. A hypothesis is just an educated guess about some aspect of reality. It is proposed by a scientist as a fact of the world, something that can be relied on to be always true within certain conditions. If the conditions are true, the hypothesis can be used to predict the future and tell us about the past.
Once formed, the hypothesis is communicated to other scientists, who test the hypothesis by experiment. The objective of an experiment is not to prove the hypothesis true; rather, the objective of an experiment is to prove the hypothesis false. If successfully proven false, the hypothesis is rejected. This is the fate of most hypotheses. The path of science is littered by the half-truths of discarded hypotheses. On the other hand, if the hypothesis survives the challenges of repeated experimentation, it becomes elevated by the community of scientists to the status of theory, and its predictions become part of scientific knowledge. This is a relatively rare phenomenon.
The falsification objective of the scientific method is a commonly misunderstood aspect of the process, but it is fundamentally important. It gives science its power over other means of understanding reality, but it also gives science its pace. It takes time to test hypotheses. The proof of a hypothesis can be shortened by increasing the number of simultaneous experiments, but only to a point. Science, like fine wine, requires adequate aging.
For all its power, the elevation of hypothesis to theory illustrates another weakness of the method: theories are created by scientists. Scientists are people, and people make mistakes. Scientists have made many. We can review examples of the most spectacular blunders of scientists later. The point is that the mistakes of science are the mistakes of people, not fallacies in the method.
So why do we trust science? Because, despite its flaws and weaknesses, science has increased our understanding of the world exponentially. But can we be misled by science? Of course we can, and we are most vulnerable when products labeled as science are not developed with strict adherence to the scientific method.
This brings us to the controversial part. Most of everything we have learned and developed in the war against COVID-19, including the tests, the treatments, and the vaccines, should not be trusted as science. In the middle of this emergency, there has not been enough time to fully study the virus and the disease by the scientific method. Rather, what we have so far are merely hypotheses: the best guesses of the smartest and brightest people in the land. To be sure, these hypotheses are our best hope in this fight against pandemic, but they should not be labeled science. There has not been strict adherence to the scientific method. So, what should we trust, what should we view skeptically, and how can we tell the difference? We will address these questions next time.
- Spread and Detection of Variants
Last time we learned that a new strain of the SARS-CoV-2 virus has emerged in London and southeast England. This variant strain, called “VOC 202012/01” or “B.1.1.7” is more infectious than the standard SARS-CoV-2. It has quickly spread to other parts of Europe, and its presence is now reported in Canada and the United States. At least two other distinct variants are reported in South Africa and Nigeria. How do we keep track of these variants, and what does their rapid spread mean?
The variants are named by adding suffixes of letters and numbers to help keep the many cataloged mutations straight. Two different systems may be used. For example, the South African variant is labeled “501Y.V2”, but it is also known as “B.1.351”. The Nigerian variant is called as “B.1.207”. Neither of these has been labeled a “variant of concern”.
A “variant of concern” is a strain is associated with differing clinical features such as greater disease severity or faster spread. “Variants of concern” will have the letters “VOC” in their name. So far, the first and only “variant of concern” is VOC 202012/01, the variant identified in London which has now spread into Europe, Canada, and the United States.
While none of the variants identified so far seem to evade detection by the PCR tests generally available to the public, these tests will not tell you whether a detected virus is one of the variants. Specialized sequencing is required to identify a virus as a variant. This testing is conducted on a regular but limited basis by the CDC, state and local health departments, and various universities.
The CDC is watching the evolution of variants closely. The concern is that increasing numbers of variants may change the way the virus spreads, may reduce detection by current tests, may create resistance to drugs such as monoclonal antibodies, or may produce a strain that evades immunity caused by vaccine or previous infection. We will watch too. As the “variant of concern” spreads into the United States, remember what keeps us safe: mask up, keep apart, and isolate when exposed.
- Viral Variant
A new variant of the SARS-CoV-2 virus is emerging in Great Britain, becoming the dominate form of the virus that causes COVID-19 in London and southeast England. What are the implications of this new variant?
The new variant has been officially named “SARS-CoV-2 VOC 202012/01.” You may also see it referred to as “B.1.1.7”, or “SARS-CoV-2 Variant” in both the popular and scientific press. This variant has a mutation in one of the spike proteins which binds the virus to human cells during the infection process. So far, this variant has not been reported in the United States.
Viral mutations are common. In fact, many different strains of the SARS-CoV-2 virus are likely to exist in the United States right now. But so far, none of these mutations has caused a significant difference in the binding capacity of the virus to human cells. At least none that we know of. Our understanding of SARS-CoV-2 continues to evolve rapidly.
The variant identified in England seems to spread more quickly in humans. The thought is that the change in spike binding protein makes it more likely for the virus to stick to human cells.
Why does increased stickiness of virus affect the virus’ ability to spread? After the virus sticks to the cells lining the inside of the nose and upper airways, the virus injects its genetic material into the human cell. This genetic material is programmed to take over the machinery of the cell, causing it to abandon its usual functions and become a virus producing factory, spewing out hundreds of new copies of the virus. These new viral copies infect other cells, either in the same body, or in bodies nearby. This accounts for the waxing of disease within a sick, infected person, and the spread of virus from person-to-person. If the virus is stickier, more human cells are taken over, and more copies of the virus are produced, making it easier for the virus to go, well, viral!
Will tests detect this new virus strain? Yes, PCR tests will, at least for now. Because PCR tests use two or three different detection targets, the change in this variant’s genetic code is not enough to evade detection by PCR tests. However, as the genetic code of the virus continues to evolve, it is conceivable that a mutation will arise that is not detected by tests currently in use, even PCR tests. Antigen tests, which already have low sensitivity, do not share the multi-targeted feature of PCR tests; therefore, even more false negative antigen test results can be expected when the variant becomes more prevalent.
Will the variant reduce the effectiveness of vaccine? The honest answer is that we really don’t know. Theoretically, this variant will not, since the vaccines released in the U.S. are polyclonal, causing the formation of antibodies to several different parts of the virus’ spike proteins. The theory is that even if one part of the spike protein changes, the antibodies will still be effective against the other parts that have not changed. But theory and reality are not the same thing. We won’t know for sure until vaccine effectiveness has been studied in populations infected by the variant.
This brings us to one final point about this viral variant. This variant is undoubtedly the first of many variants to come, and the answers for these yet-to-be-seen variants may be different than the answers for this one. Viruses want to survive. Just as the use of antibiotics causes the emergence of antibiotic resistance in bacteria, the use of vaccine will favor viral mutations that evade vaccine-induced immunity. Variants will emerge that are unaffected by vaccine.
The pandemic is a war, both metaphorically and really. Our best defense is the practice of what we know reduces spread: mask up, keep apart, and isolate when exposed. We will prevail. But it’s still too early to celebrate victory.
- Mask Up!
Individuals exposed to someone infected by SARS-CoV-2 should be quarantined to slow the spread of COVID-19 and keep our loved ones safe. However, being quarantined is a lot like being in jail. How can we avoid drawing this card?

We have learned a lot about the spread of SARS-CoV-2 in the last ten months. Those exposed to individuals infected by the virus are at risk of becoming infected themselves. According to the CDC, an exposure is an encounter of less than 6 feet apart and more than 15 minutes long when one or both individuals are not wearing face masks. By this definition, wearing a mask and keeping your distance from those not wearing masks prevents exposure to SARS-CoV-2.
Does that mean that you will never get SARS-CoV-2 if you wear a mask? No, wearing a mask cannot prevent all SARS-CoV-2 infections, but it will dramatically reduce your risk of infection and your risk of being dragged into quarantine jail.
How do we know that masks work? The CDC has published evidence for the effectiveness of masks. To this list, I add two observations from my own experience.
In the hospitals where I work, all physicians, staff, patients, and visitors are required to wear masks. Although some individuals have become infected with SARS-CoV-2 during the pandemic, contact tracing demonstrates that individuals were infected outside of work. I have not observed “hot-spots” of infection in clinical areas where these precautions are practiced. This, despite treatment of hundreds of patients with COVID-19 at these hospitals.
The second point is the absence of flu in Texas this December. By this time of the year, flu season is generally in full swing. In mid-December, the laboratories where I work have usually detected many positive flu samples. However, this year these same laboratories have yet to see their first positive flu test. This is not for lack of testing for flu. Since October, every rapid PCR test for SARS-CoV-2 has included a test for flu.
Why is this observation relevant? Flu is a respiratory illness transmitted in much the same way as SARS-CoV-2. What prevents spread of coronavirus also prevents the spread of influenza virus. With masking orders in place, the spread of flu has dramatically reduced.
If masking has effectively stopped the spread of flu, why is COVID-19 surging? Coronavirus is much more infectious than flu. The point is that masking reduces all disease that spread by the airborne route. Imagine what the surge would be like without masking?
In Texas, we love to wear our boots and hats. This year, we’ve learned to love our masks, worn all the way up, covering the nose and mouth. Be safe during the coming holidays. Mask up, y’all!
- Quarantine
In guidance updated December 2, 2020, the CDC adjusted quarantine period for asymptomatic individuals. Today we consider these latest quarantine recommendations.
Before we do, we must first discuss what it means to quarantine and the conditions that trigger a quarantine. Quarantine separates an individual who may have been exposed to SARS-CoV-2, the virus that causes COVID-19, from others to prevent further spread of the virus. Simply stated, quarantine means stay home and stay away from others. If you live with other people, keep to a separate room. If you must be in the same room with someone else, stay 6 feet away, wear a mask and make sure everyone else does too. Generally, if one person in a household is quarantined, all persons in that household should also quarantine.
You must quarantine when (1) you have COVID-19, (2) you first positive test for SARS-CoV-2, or (3) you are exposed to someone infected by SARS-CoV-2. An exposure is an encounter of less than 6 feet apart and more than 15 minutes long when one or both individuals are not wearing face masks.
The standard quarantine period for asymptomatic individuals is 14 days. This recommendation comes from the maximum observed time between exposure and development of symptoms, known as the incubation period. The incubation period is less than 14 days for most infected individuals, with 5-7 days being average.
The new CDC guidance lists two situations when the quarantine period can be shortened to less than 14 days. If no symptoms develop, the quarantine can be ended after 10 days without testing for SARS-CoV-2. But if the person tests negatively for SARS-CoV-2 on or after the 5th day of quarantine, and if the person never develops symptoms, then the quarantine period can be ended after day 7. For the purposes of counting days, the exposure day is considered day 0.
Immediate testing at the time of exposure is not recommended. Testing prior to 5 days after exposure does not shorten the recommended quarantine period and could lead to a false perception that the exposure did not lead to infection, perhaps promoting risky behavior.
The quarantine period is different if you have symptoms. For persons with mild illness, the quarantine period is 10 days from the onset of symptoms or 24 hours since the last fever without use of fever-reducing medicines such as Tylenol, whichever is longer. Generally, a mild illness is one that does not require hospitalization. If hospitalization is required, the quarantine period may be 20 days or more, depending on the advice of your doctor.
Following these updated quarantine guidelines slows the spread of the disease and keeps your loved ones safe. However, wearing a mask and staying away from people who are not wearing masks minimizes the risk of exposure in everyday encounters. More on masks next time.
- Accuracy, Precision and Predictive Value
We want accurate tests, don’t we? By that, don’t we mean that we want precise test results? Well, not exactly. Before we leave the subject of laboratory statistics, there are a few more words we need to learn.
Accuracy is the ability of a test to aim for the target. Visually, accuracy looks like this:

Even though none of the shots hits the bullseye, we can tell where the shooter is aiming.
Precision is the ability of a test to get the same answer repeatedly, illustrated like this:

Even though none of the shots hits the bullseye, all of the shots go to the same spot.
Putting these terms together, we can describe different aspects test performance. Poor accuracy and poor precision look like this:

The shots are not centered on the bullseye, and they do not hit the same spot. Together, favorable accuracy and precision can be illustrated like this:

All the shots hit the bullseye, repeatedly. This is what an accurate and precise test looks like, too. Accuracy and precision are both desirable but different aspects of test systems.
But are accuracy, precision, sensitivity and specificity enough to interpret tests? Consider the case where these aspects of a test system are optimized. In other words, the test is highly accurate, precise, sensitive and specific. But what if the condition being tested for is not prevalent in the tested population. Prevalence is the percentage of people in a given population who have the condition of a positive test. Consider a test is 99.99% specific. That means that for every 10,000 results, there is only 1 false positive. But let’s say that the condition exists in the population at a rate of only 1 per 10,000 individuals. In other words, out of 10,000 results, there is only one true positive result. But we’ve already said that out of 10,000 tests, there will be one false positive result. Therefore, if we get a positive result, there a 50% chance it’s the false positive, not the true positive. That is what is meant by the term positive predictive value.
Both positive and negative predictive values can be measured. These are expressed mathematically as PPV = TP / (TP + FP) and NPV = TN / (TN + FN), respectively. It’s okay to skip the math; just remember that predictive values are dependent on the prevalence of the condition; sensitivity and specificity are not.
Predictive value is important for test interpretation but should not be used for test selection. Instead, sensitivity, specificity, accuracy and precision should be used to guide appropriate test selection. These are the terms by which test systems are judged, and the key aspects of test performance analyzed by the FDA before tests are approved for use in the United States.
- Sensitivity and Specificity
We want tests that are highly sensitive and highly specific for the condition being tested, but that is not always possible. Often, we must sacrifice one for the other. Simply stated, negative results can be trusted when there is high sensitivity, and positive results can be trusted when there is high specificity. So, we have to ask: is it better not to miss negatives or positives?
There is not usually a neat separation between healthy patients and patients with disease. Instead, patient populations exist in overlapping distributions, which can be illustrated as follows:

The vertical blue line represents the cutoff between positive and negative test results. In this illustration, the cutoff is placed in a compromise position between the two populations, creating a group of false negatives (FN) and false positives (FP).

If a test is highly sensitive, the cutoff is shifted to the left, eliminating false negative results, but increasing the number of false positive results.

If a test is highly specific, the cutoff is shifted to the right, eliminating false positive results, but increasing the number of false negatives. As we have discussed previously, this is the situation with antigen tests for SARS-CoV-2.
When screening large populations for disease, it is important not to miss possible positives, so we choose a test that highly sensitive. We do not want any false negatives. False positives can be sorted out later; this is just a screen after all. On the other hand, it is important that confirmatory tests have high specificity. When we are confirming disease in a population selected by a screen, we want to eliminate false positives.
If the goal of testing for SARS-CoV-2 is to avoid false negative results, favor sensitivity over specificity. But this trade-off is not necessary with all test systems. PCR tests increase sensitivity by amplification and increase specificity with detection probes unique to the virus. The result is a separation between populations, increasing specificity and sensitivity at the same time:

Are sensitivity and specificity the only considerations when evaluating a test? No, it is more complicated, but I am sure you guessed that. We will talk about other measures of test systems and the results they produce next time.
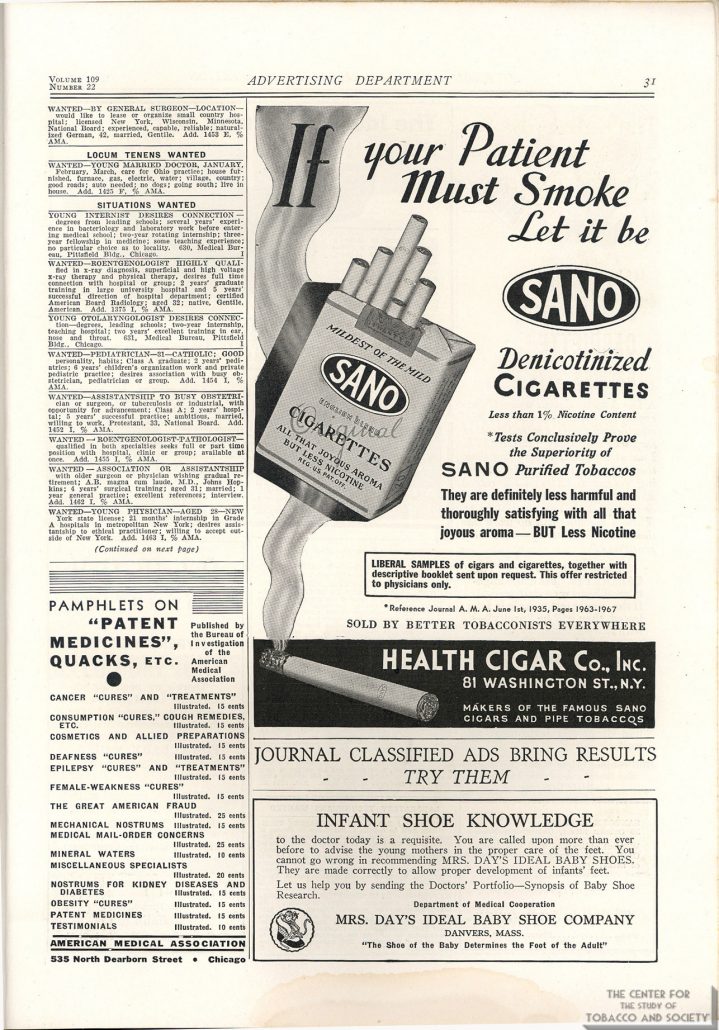{kind=link}
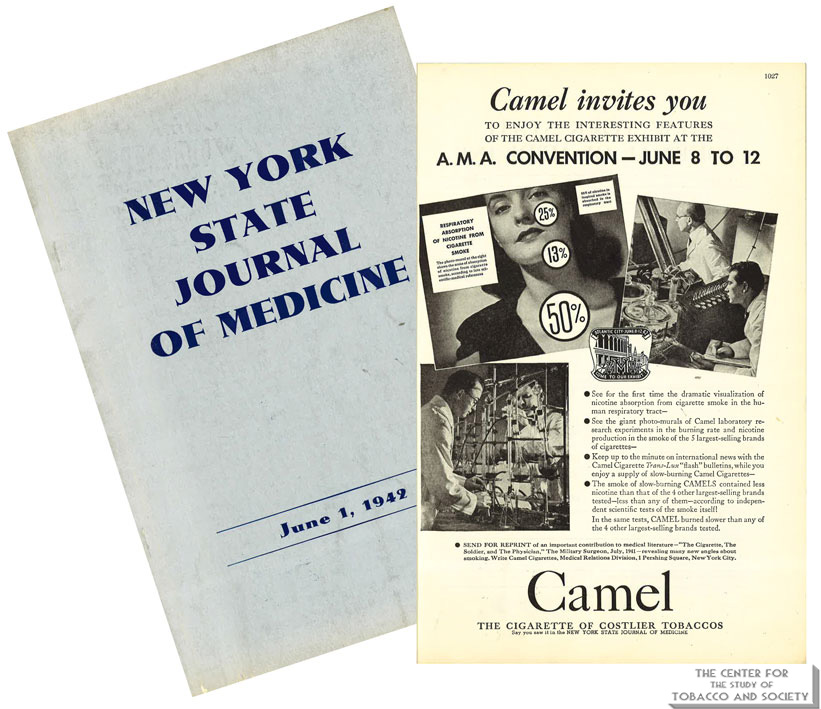{kind=link}
{kind=link}
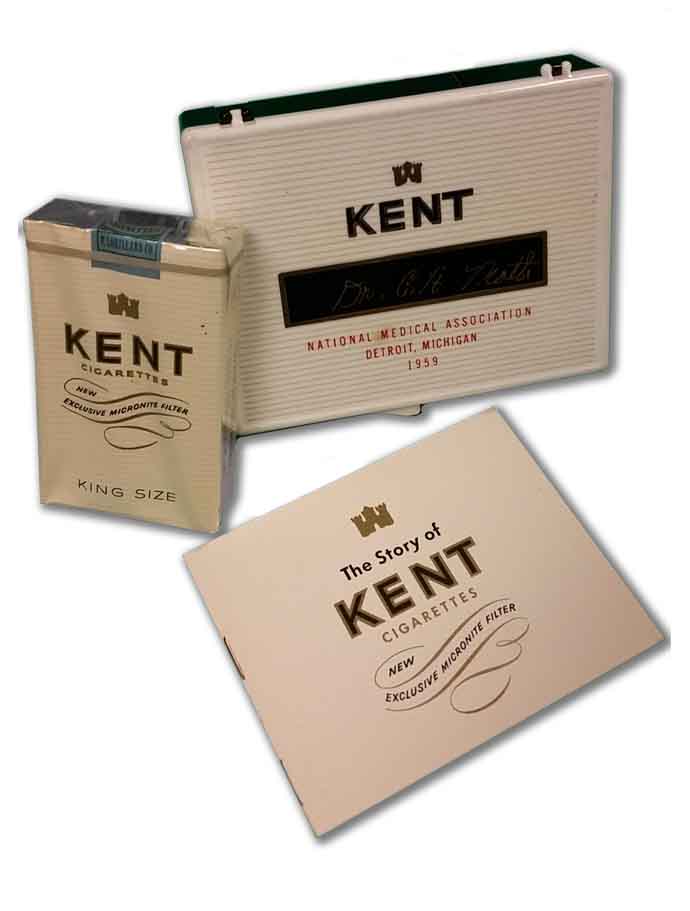{kind=link}
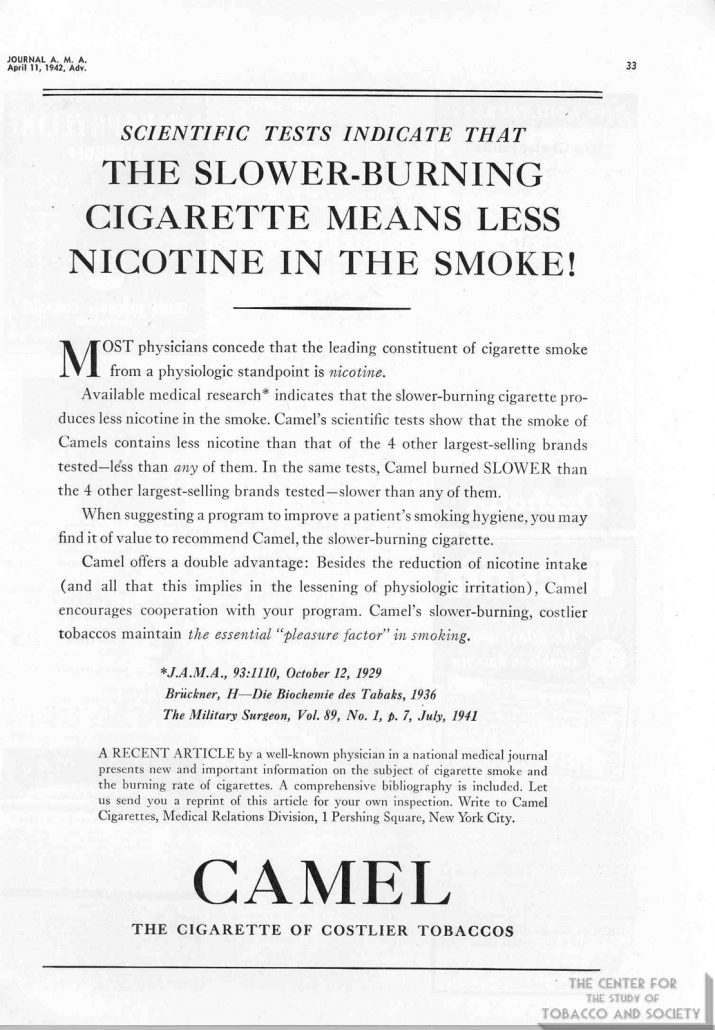{kind=link}
{kind=link}
{kind=link}
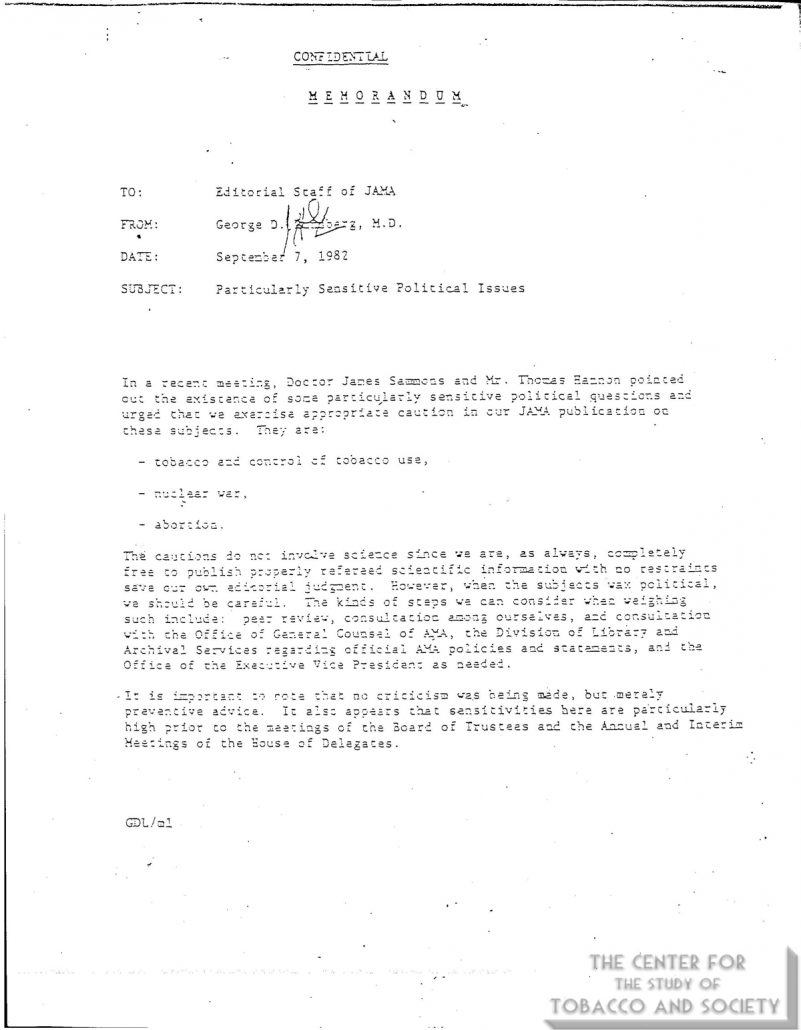{kind=link}
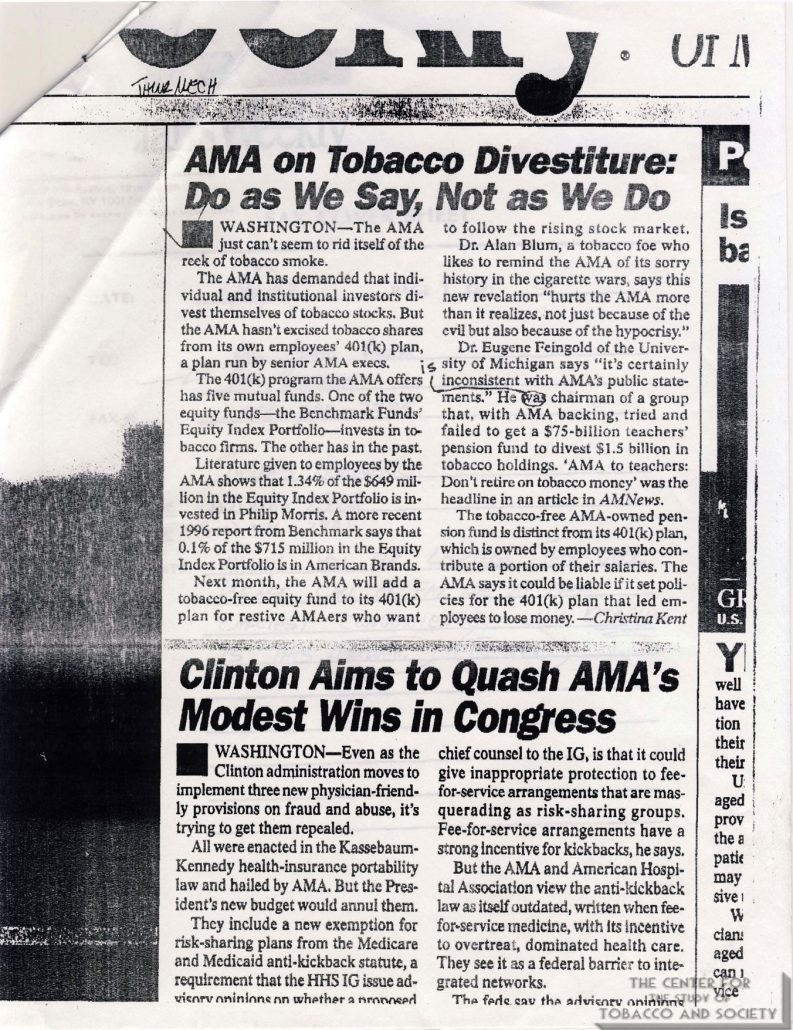{kind=link}
{kind=link}
{kind=link}
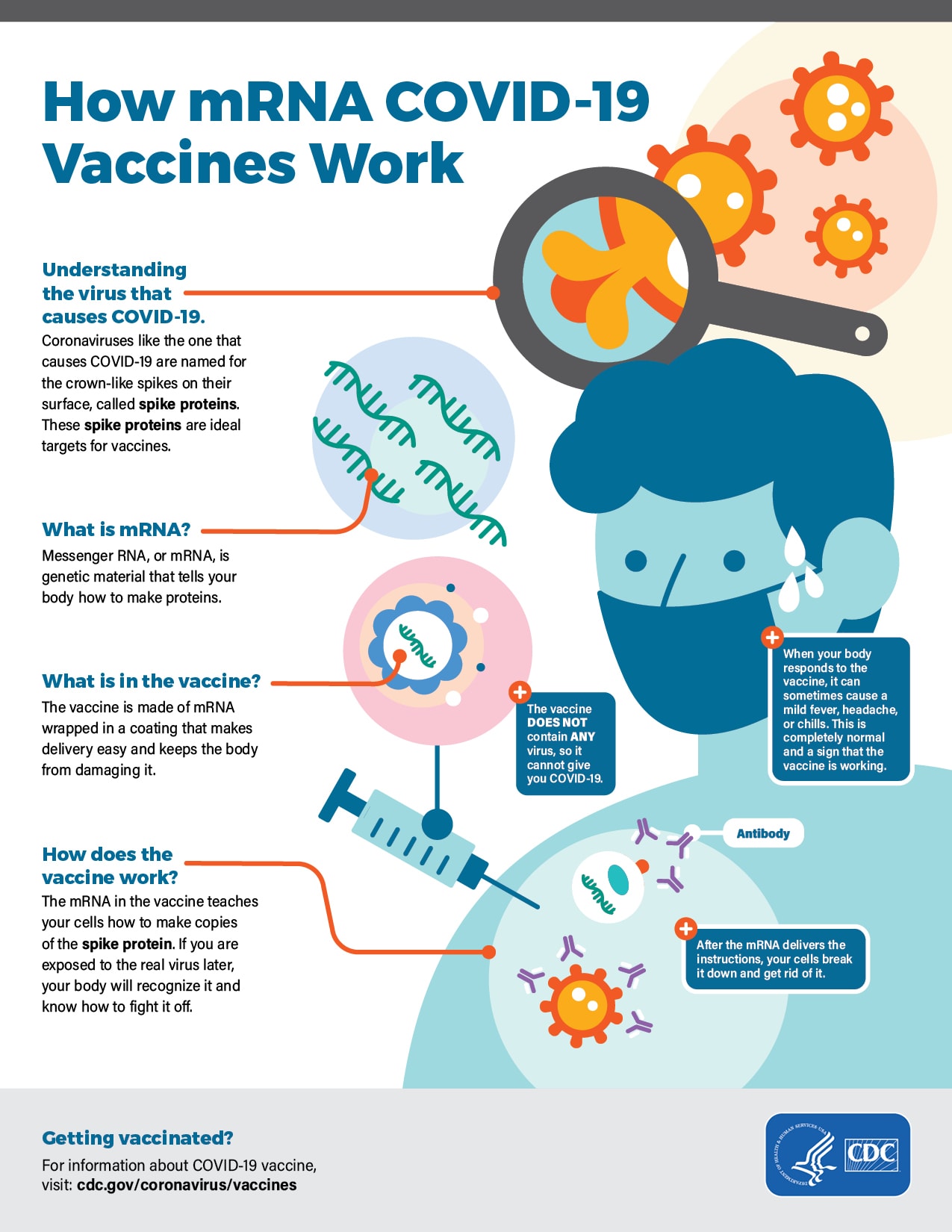{kind=link}
{kind=link}