Connecting people with information needed to live their best possible lives.
- Pathology in Pandemic
Much attention has been given to testing this year, so much attention that the subject has become confused and misunderstood by many. What is testing? Who should be tested and when? What kinds of tests are there? What is the meaning of positive and negative results? These and other questions should and do have clear, simple answers. But in the noise that accompanies the pandemic, clarity is lost. The result is widespread and profound misunderstanding of the utility and application of diagnostic testing in our fight against COVID-19, the disease of the pandemic.
A clear understanding of testing is important. Diagnostic excellence is the foundation of excellent treatment outcomes. Clarity of understanding must precede planning and execution. Tragic accidents are more likely in the fog of distorted perceptions. Using my perspective and experience as a clinical pathologist, my only purpose here is to make the use of laboratory testing as clear and understandable as possible.
During the nine years I spent in medical school and pathology training at the UT Southwestern Medical Center at Dallas, I had the good fortune to encounter some of the most renowned researchers and practitioners of my profession, men and women whose mind-power far exceeds my own, but whose common sense approach to solving diagnostic problems had a profound and enduring impact on my career in pathology. Added to the formal education and training, I have spent more than 25 years in practice at a mid-sized community hospital as pathologist and laboratory medical director. My career has driven home fundamental lessons of laboratory medicine: when it is important to test, when it is better not to test, and how misunderstanding of test results can lead well-meaning doctors astray, to the detriment of their patients.
In the blogs that will follow, I will sacrifice scientific rigor for clarity and understandability. I am a practitioner, not a scientist. Accordingly, my emphasis is on the use and pitfalls of diagnostic tools, not the precise science that makes the tools possible. The science is fascinating, and, at a certain level, necessary for the appropriate use of the clinical laboratory. But a rigorous understanding of science is not the same as mastery of use of the diagnostic tools created by science any more than the knowledge of piano construction confers the ability to play. Incidentally, I firmly believe that even our most fundamental scientific theories should never be considered true and unchangeable representations of reality, but rather artificial constructions that make certain phenomena understandable and predictable. However, as I am not a scientist, I am neither a philosopher, so I leave to the philosophers the further contemplation of these compelling yet impractical notions. For now.
- Names to Know
Before we can talk about testing, we must first agree on terminology. The official name of the disease of the pandemic is COVID-19, short for Coronavirus Disease of 2019. The official name of the virus that causes COVID-19 is SARS-CoV-2, so named because it is a coronavirus (“CoV”) that produces Severe Acute Respiratory Syndrome (“SARS”). The “2” is tacked on the end to distinguish this virus from the SARS-producing coronavirus that caused the outbreak in 2003; that virus is now called SARS-CoV-1. I am just reporting here—no one asked for my help to come up with these names.
The relationship of SARS-CoV-2 to COVID-19 is the same as the relationship of HIV to AIDS. The first is the name of the virus; the second is the disease that may be caused when infected by the virus. I said “may” because being infected by the virus is not the same as having the disease. In order to have the disease, you must test positive for the disease-causing virus, and you must also have the disease’s defining symptoms. In the case of AIDS, the defining symptoms include co-infection by at least one of a long list of “opportunistic organisms”, organisms that take advantage of a weakened immune system. In the case of COVID-19, criteria for disease requires symptoms of respiratory illness which may range from “cold symptoms” to pneumonia. A person infected by SARS-CoV-2 who does not have those symptoms does not have COVID-19.
It is important to note that there is no laboratory test for COVID-19. Instead, the laboratory tests for the presence of the virus that causes COVID-19 (i.e., SARS-CoV-2) or the body’s response to infection by that virus. Next time, we will discuss the various tests available for detection of the virus or the body’s response to infection.
- What is a COVID Test?
It may surprise you to learn that there is no test for COVID-19, the disease of the pandemic. Instead, tests look for SARS-CoV-2, the virus known to cause COVID-19, or the body’s response to SARS-CoV-2. These different tests are all commonly (but inaccurately) called “COVID Tests”, probably because it is easy to say.
Tests for SARS-CoV-2, like all laboratory tests, have two phases: pre-analytic and analytic. The analytic phase occurs within the walls of the laboratory at the testing bench. The pre-analytic phase includes all activities that occur up to the time that the specimen is placed on the analyzer in the laboratory, including specimen collection and transportation.
A direct test for the virus requires collection of a sample by swab. The greatest concentration of virus is found in the back of the nose (“nasopharynx”), so that is where most swab collections are taken, but virus may also be found in other places in the body, including the middle portion of the nose and in saliva. Collection can be uncomfortable. There is no blood test that can directly detect the virus. Most drive-through “testing” centers are actually drive-through collection centers since very few actually analyze samples on-site. Most of these sites send their collections to a large central laboratory for analysis.
A test for the body’s response to viral infection is known as an antibody test. The antibody is present in the bloodstream, so a blood sample is all that is needed for this test. There is a time lag between infection and detectable antibody in blood, so an antibody test is not useful to detect patients that might infect others. Therefore, antibody tests have had limited utility during the present pandemic.
The most accurate test for SARS-CoV-2 is the PCR test, which will be the subject of the next blog.
- PCR Tests
There is no test for COVID-19, the disease of the pandemic. Instead, tests look for the presence of SARS-CoV-2, the virus known to cause COVID-19, or the body’s response to SARS-CoV-2. This last group, known as “antibody” tests, have found very little utility during the pandemic. There are different kinds of tests in the first group, the tests for the virus, and the reliability of these tests vary widely based on methodology. Today, we will discuss the gold-standard method: polymerase chain reaction, known as “PCR”.
PCR is a several step process. It begins by exposing the sample to the components necessary for replication of nucleotide segments. Nucleotide segments are pieces of DNA or RNA which carry the genetic material of cells. By exposing the sample in this environment to a series of 30 to 40 heating and cooling cycles, all of the DNA or RNA sequences contained in the sample are amplified—and not just 30 to 40 times, but one to 230 to 240 times. That’s one billion to one hundred billion! This produces a highly sensitive test able to detect minute quantities of genetic material.
But, you might ask, if all genetic material is being amplified, won’t other genetic material in the sample not related to the virus be amplified also? Yes, it will, but that’s where the second part of the test becomes important.
Probes are incubated with the amplified sample that bind to a specific nucleic acid sequence that is known to be unique to the target—in this case the SARS-CoV-2 virus. If that sequence exists, then the probe binds, and a signal is sent to the test system. If the sequence doesn’t exist, then there is no signal. It’s like looking for a specific password to a website among all the passwords that could possibly be entered.
But, you might ask again, couldn’t that nucleic acid sequence exist in the sample just by chance? That would be like you guessing the password to a billionaire’s bank account; unlikely, but not entirely out of the question.
That is why PCR tests for SARS-CoV-2 include a second set of probes, specific a different nucleic acid sequence that is also unique to the virus. Only if both signals are detected is the test positive. Some PCR tests even use a third set of probes. The result is a highly sensitive (meaning detection of tiny amounts of viral RNA) and a highly specific (meaning false positive rates close to zero) test system.
But like any human endeavor, PCR is not perfect. False negative results can occur if the sample is improperly collected, resulting in no viral RNA to amplify. Sloppy analytic practices can lead to false positive results by a process referred to as “carry-over”—literally, the genetic material from one sample is carried-over to another sample.
There is another source of apparent false positives: a patient who is not sick and not infectious but has a positive test. I call this pseudo-false positive, because it’s not a false positive result at all. Instead, it’s a failure to interpret the result correctly. Remember that laboratories do not test for the COVID-19 disease; they test for the SARS CoV-2 virus itself, and in the case of PCR tests, for viral RNA. Viral RNA is known to persist in detectable quantities for weeks, even months, after the patient has recovered from the disease. How is this possible? Because to be infectious, the virus must have the genetic code wrapped in a capsule that binds to human cells. Without the capsule, the RNA is inert. When the body clears an infection, it denatures the capsule. Remnants of the viral RNA persist for a long time afterwards, just like a bombed-out city after a war.
It gets even more complicated. There are tests which have unfortunately received Emergency Use Authorization (EUA) from the FDA which are not as sensitive or specific as PCR tests. These are many of the super rapid tests (<15 minutes), some of which have sensitivity rates as low as 67%. These tests are known as “antigen” tests, and we will address these tests soon. Next, we will discuss the meaning of positive and negative tests.
- What Do Test Results Mean?
We want a test to tell us whether someone has COVID-19, but that test does not exist. Instead, laboratory tests look for the presence of SARS-CoV-2, the virus known to cause COVID-19. A positive test does not necessarily mean that someone has COVID-19 and a negative test does not always mean that someone does not have COVID-19. How can this be? And if this is true, what is all the fuss about testing?
Let me be clear. Testing is the most important tool available to determine who has COVID-19 and who does not. But it is not quite as simple as “positive” equals COVID-19 and “negative” does not. At least not quite. The test must be interpreted, and to do so, a few simple nuances must be considered.
The most reliable test uses PCR methodology, which includes both amplification and detection steps, making it highly sensitive and specific for the detection of virus.
A negative PCR test means that an individual is not currently infected and has not been recently. But a negative PCR test cannot be used to predict the future. In other words, a negative test last week does not prove someone is virus-free today. Instead, a negative test simply tells us the last time a person was known to be negative for virus. The significance of a negative test result diminishes rapidly as the collection time fades into the past.
A positive PCR test means that the person tested is or has been infected by the virus. If the individual is also symptomatic, we can say the person has COVID-19. That patient is also infectious (i.e., can spread the virus to others), and should be considered infectious for at least ten days after the first positive test, or for 24-hours after symptoms resolve, whichever is longer.
Our best understanding is that a person does not need to have COVID-19 to spread the virus to others. Most people test positive five to seven days after exposure, but they can infect others for ten days from time of exposure, longer in exceptional cases. That is why a person is considered infectious and instructed to quarantine for at least ten days after the first positive test, even without symptoms. A PCR test may continue to be positive for weeks to months after infection, making it impossible to know whether asymptomatic people with a first-time positive test are newly infected or were infected in the past. Because we cannot know when the person became infected, the asymptomatic individual should be considered infectious for at least ten days after the first positive test.
Another consequence of the persistence of positive PCR tests after the infection has cleared is that there is no need to require a negative test to prove an individual is no longer infectious. After the appropriate amount of time has passed since the first positive test and/or resolution of symptoms, an asymptomatic individual should be considered virus-free for at least three months.
If you may have been exposed, when should you test? A test for SARS-CoV-2 becomes positive 2 to 14 days after infection, with most patients turning positive five to seven days later. Most authorities suggest testing no earlier than five days after possible exposure, unless you have symptoms earlier. But if you have to wait five days, should you even test at all? Whether you test or not may be a decision that addresses your peace of mind more than anything else. The most important thing you can do if you think you may have been exposed is to self-quarantine for two weeks. That is how you keep others safe and stop the virus spread.
- COVID-19 Penetrance
Why do some people become seriously ill and even die after infection by SARS-CoV-2 and other people have no symptoms at all? Why do some infected people get COVID-19 and others do not? These are vexing questions that do not have satisfying answers. We will learn much about COVID and the virus that causes it in coming months and years, but today we will consider what is currently known about the penetrance of COVID-19.
Penetrance is a medical term used to describe the relationship between the number of people with a disease and the number of people with the condition causing that disease. If most people with the condition develop disease, the disease has high penetrance. Incomplete penetrance is the term used to account for the fact that not everybody with a condition suffers from the disease caused by that condition. Although these terms have roots in clinical genetics, we may apply these concepts to viral infections. For example, without treatment, most people infected by HIV develops AIDS, but only 30% of people infected by the Hepatitis B Virus (HBV) develop acute hepatitis. (Of course, I must add that with current anti-retroviral therapy, many fewer people with HIV infection develop AIDS.) We can say that among people infected by the causative virus, AIDS has higher penetrance than Hepatitis B. I am sure any number of researchers who can tell you why this is. I cannot. But I can tell you that it happens.
In the case of COVID-19, it seems that penetrance is relatively low. In fact, according to the CDC’s best estimates, the rate of asymptomatic infections is about 40%, meaning that COVID-19 penetrance is about 60%. But that is an overall rate for all patients. Can we identify who is at higher risk for disease after infection?
Although we cannot accurately predict which individuals will get severe disease after infection, we can identify populations who are at greater risk. For example, advanced age is clearly associated with risk of severe disease, and, therefore, higher penetrance. Using the best CDC estimates, about one in twenty infected people over 70 dies of disease, compared with one in 200 aged 50-69, one in 5,000 adults 20-49, and one in 35,000 young people under 20.
There are other conditions that predict serious symptoms after infection. Obesity, diabetes, COPD, heart disease, pregnancy, cancer, sickle cell disease, high blood pressure, smoking and immunodeficiency are all associated with more severe disease, and therefore, higher disease penetrance. But it’s not just the elderly or chronically ill who get sick; young, healthy individuals can and do get seriously ill. Even if you are in a group that has a low disease penetrance, if you get seriously ill, the penetrance for you is 100%.
Because there are still so many unknowns, it is more prudent to avoid infection than “get it over with.” Wear your mask in public, avoid social gatherings, and keep your distance. Stay safe, and help keep others safe too.
- Antigen Tests
Elon Musk recently tweeted that he was tested four times in the same day. Two tests were positive, and two tests were negative. How can this be?
Mr. Musk was tested with the BD Veritor Plus rapid antigen test for SARS-CoV-2. BD Veritor is one of several SARS-CoV-2 antigen tests made available in the United States by an Emergency Use Authorization (EUA) with the FDA. While PCR tests have some limitations, antigen tests are fraught with many more challenges that bring their results into question.
First the good news. Antigen tests are cheap, plentiful, and rapid, usually providing results in 15 minutes or less. And, with one exception, all antigen tests can be performed in laboratories operating under a CLIA Certificate of Waiver, meaning that they can be performed by personnel with very little education in laboratory science.
So what’s the bad news? I see three major problems with antigen tests: the test process, the lack of amplification, and poor sensitivity.
The antigen tests from different vendors all follow, with minor variations, the same process. A sample is collected on a swab, usually from the back of the nose (nasopharynx), and the swab is placed in an incubation well on the test device. A few drops of reagent containing antibodies against the target (in this case, the SARS-CoV-2 virus capsule) are added. If the antibodies bind to the target, a signal is sent to the test system. This signal is usually a color change. The whole process is very much like a home urine pregnancy test.
Well, what could go wrong with that? Strong lines are easy to see, but what about faint lines? Where is the cut-off between positive and negative? Some vendors include a reader calibrated to take the guesswork out of reading results, but you begin to see the problem. The test system introduces an element of subjectivity and operator technique that varies from tester to tester, and these variations impact test results. Recall that most of these tests are intended to be performed by personnel with very little training in laboratory medicine.
This process lacks the amplification step of PCR. That means when the swab is scraped against the back of the nose, what rubs off is all that you have for the test. If you happened to not scrap off enough virus in an infected person, too bad—the test will be negative.
And that brings me to the final problem with antigen tests: low sensitivity. According to the FDA submissions by BD, the antigen test used on Mr. Musk has a sensitivity that may be as low as 67%. What does that mean? Sensitivity of 67% means that one out of every three infected patients tests negative with the system. That’s right: wrong answers one-third of the time! And that is in the best of circumstances, using data that the manufacturer chose to submit to the FDA. These tests are not always used in the best of circumstances; remember, the test is approved for use by personnel with very little education in laboratory science.
BD makes the following statement in its submission to the FDA: “Negative test results do not preclude infection and should not be used as the sole basis for treatment or other patient management decisions, including infection control decisions, particularly in the presence of clinical signs and symptoms consistent with COVID-19, or in those who have been in contact with the virus. It is recommended that these results be confirmed by a molecular testing method, if necessary, for patient management.” Mr. Musk’s experience is not surprising.
My colleague says she has a Magic 8–Ball on her desk that is a lot like an antigen test: it’s cheap, plentiful and rapid. And, she says, it gives about as many correct answers. I agree.
- Antibody Tests
There is no test for COVID-19. Instead, testing focuses on detection of SARS-CoV-2, the virus known to cause COVID-19 or the body’s response to infection. Today we will discuss antibody tests, the blood tests used to detect past infections.
Part of a healthy immune response to infection by any virus is the formation of antibodies. Antibodies are made in plasma cells, a special type of lymphocyte, in response to an assault by a foreign pathogen such as a virus. The immune response is amazing. Once plasma cells “learn” how to identify the virus, they crank out millions of these little molecules which coat the surface of the virus, flagging them as “enemy”, and directing other cells of the immune system to isolate and eliminate them. Once the infection is cleared, the plasma cells “remember” the code for that virus so they can be quickly recruited to make more antibody if the same infection occurs in the future. This memory eliminates the time-consuming “learning” step. This simple process explains why most people only get chickenpox once and explains how vaccines can protect children from mumps and measles.
The first antibodies produced after infection are known as IgM Antibodies. These are large pentamers, basically 5 antibody units brought together like a snowflake. IgM antibody production is replaced with IgG antibody production generally after about a week, but the time varies by individual and virus. IgG antibodies are produced for weeks to years after infection, again depending on the individual and the virus. Other antibodies are produced by the immune system, but IgM and IgG are most useful in viral serology. These antibodies are found in the blood stream, so a simple blood test can detect a variety of antibodies, including antibodies to SARS-CoV-2. It is thought that antibodies to SARS-CoV-2 is what makes convalescent plasma an effective treatment for severe COVID-19.
There are several facts to keep in mind when interpreting antibody test results. First, antibody tests tell us about past infections, not active infections. Second, the antibody form tells us whether the infection was recent or distant. IgM antibodies are made first but go away, so detection of IgM antibodies means the infection was recent. IgG antibodies are made last but stay around for a long time. Detection of IgG without IgM means that the infection occurred in the more distant past, at least three weeks ago, and detection of both IgG and IgM means the infection occurred in the transition period.
Antibody tests use an immunoassay methodology, which basically uses antibodies to detect antibodies. Many of these tests have good specificity and sensitivity, but they are not perfect. Cross reactivity and interfering substances can cause false positive and false negative results in the best of circumstances. But we are not in the best of circumstances. All SARS-CoV-2 antibody tests are available in the U.S. by an emergency use agreement (EUA) with the FDA. Rigorous studies demanded by the FDA approval process have not yet occurred.
So, if you are positive for SARS-CoV-2 antibody, will you always be? Don’t know. If you are positive for SARS-CoV-2 antibody are you immune to COVID? Don’t know. It is simply too soon to define the body’s usual response to infection and its implication for future infection.
What can we learn from antibody tests? If your antibody test is positive, you probably had a SARS-CoV-2 infection in the past, even if you do not remember being sick. If you do not have symptoms, and you have not been around someone with COVID-19, then you are not likely to have a current infection. Continue normal activities, but with vigilant precautions. Wear a mask and social distance. These precautions reduce the spread of the disease.
- Convalescent Plasma
What is convalescent plasma and how can it help someone with COVID-19?
Most bacterial infections can be treated effectively by antibiotics, but these drugs are not effective in most viral infections. To be sure, anti-viral therapy can help control diseases caused by certain viruses. For example, antiretroviral drugs such as AZT are beneficial to those infected by HIV. Anti-influenza drugs such as Tamiflu can reduce the severity of disease caused by Influenza virus. Acyclovir is used to control the symptoms of herpes simplex (“cold sores” and “genital herpes”) and herpes zoster (“shingles”). But unfortunately, most viruses cannot be cleared by drugs.
Ebola is an example of a virus for which there is no effective drug therapy. Endemic in west Africa, Ebola virus disease (EVD) has a death rate of about 50%. Without an effective drug to treat Ebola infections, doctors treating EVD had little to offer. Several years ago, researchers hypothesized that there might be something in the blood of patients who survived Ebola virus infection that could help patients with EVD. Sure enough, patients who received plasma donated by people who had survived Ebola had a small but significant reduction in deaths compared to those who did not.
Why did this work?
The theory is that Ebola virus disease survivors form antibodies that help their bodies fight the infection. These antibodies persist in the plasma (the liquid part of blood) of survivors for a long time after infection, and these antibodies are transferred to the patient through a plasma transfusion. But this is just a theory. Although there are lots of reasons to believe this theory is true, it has not yet been proven. As I am writing, convalescent plasma transfusions are experimental.
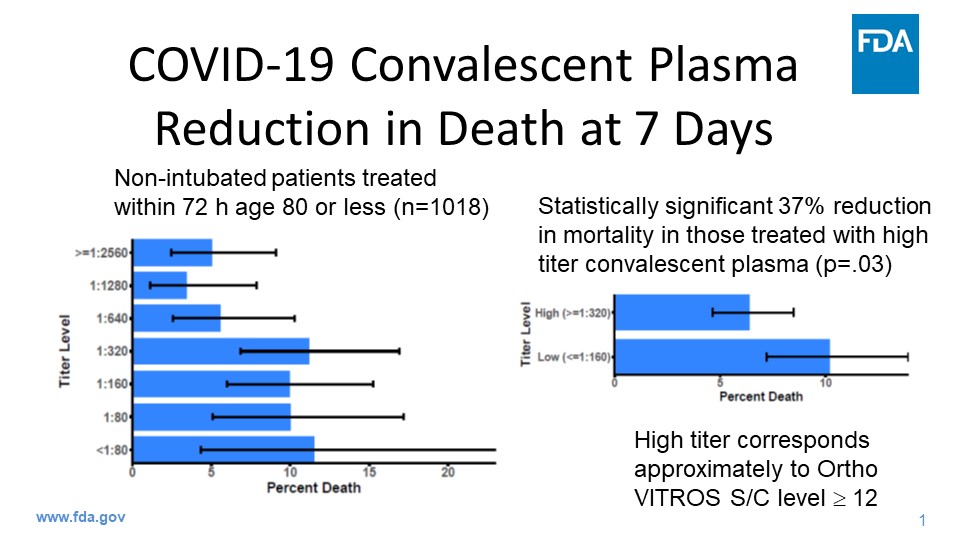
Early in the COVID-19 pandemic, doctors found themselves in a similar situation. Without an effective drug therapy, many began to use convalescent plasma as an alternative, but unproven treatment for serious disease. In early April, the U.S. government announced a partnership with the Mayo Clinic to facilitate availability of convalescent plasma to COVID-19 patients in an unprecedented nationwide experimental program. The project, known as US COVID Plasma, enrolled more than 100,000 patients. Although it will take years to fully analyze the data collected, initial results are overwhelmingly positive. In patients with serious COVID-19, the transfusion of convalescent plasma is associated with a 37% reduction in mortality. On August 23, the FDA announced an emergency use authorization (EUA) for convalescent plasma, making the treatment available to patients not enrolled in a study. Convalescent plasma has become one of the most important therapies available to treat life-threatening COVID-19. My colleagues believe it has saved countless lives. So do I.
Patients who have recovered from COVID-19 can help others who are sick with a simple plasma donation. In fact, each plasma donation can be divided into four doses, potentially helping four people currently suffering from the disease. If you have tested positive for SARS-CoV-2, please consider donating at your local blood center. You’ll be someone’s hero.
- Choosing Tests
The limits of my language mean the limits of my world.
-Ludwig Wittgenstein, 1918.Throughout the pandemic of 2020, the vocabulary of laboratory medicine has been used indiscriminately and imprecisely, resulting in muddled communication and poor decisions. Today we will discuss basic terms used to evaluate laboratory tests so that you can address these issues confidently and intelligently.
Reduced to its simplest possible terms, tests are measured by how good positive and negative results correlate to the presence or absence of the condition being tested. Tests are either positive or negative, and patients either have the condition or not. True positive results match a positive patient condition; false positive results are positive even though the patient does not have the condition. Similarly, true negative results match a negative patient condition, and false negative results are negative even when the patient has the condition. We can visualize these terms with a simple matrix:

In the case of COVID-19, laboratories test for the presence of SARS-CoV-2 in patients who may or may not be infected by the virus. Using this example, we can rewrite the matrix:

Adding the number of true positives and false negatives, you get the number of infected patients. Similarly, the number of uninfected patients is the false positives plus true negatives. Sensitivity, the measure of the test’s ability to detect infection, is the number of true positives divided by the number of infected patients: TP/(TP+FN). Sensitivity is low when there are many false negatives, but it gets close to 100% when false negatives are rare. A highly sensitive test system minimizes false negatives; when the test result is negative, you can believe it is true.
Specificity is the measure of the test’s ability to detect nothing but infection, is the number of true negatives divided by the number of uninfected patients TN/(TN+FP). Specificity is low when there are many false positives, but it gets close to 100% when false positives are rare. A highly specific test system minimizes false positives; when the test result is positive, you can believe it is true. Obviously, good test systems aspire to be both highly sensitive and specific, but like so many things in life, having both at once is often impossible. Trade-offs are inevitable. So how do we decide which is more important? We will discuss that next time.
- Sensitivity and Specificity
We want tests that are highly sensitive and highly specific for the condition being tested, but that is not always possible. Often, we must sacrifice one for the other. Simply stated, negative results can be trusted when there is high sensitivity, and positive results can be trusted when there is high specificity. So, we have to ask: is it better not to miss negatives or positives?
There is not usually a neat separation between healthy patients and patients with disease. Instead, patient populations exist in overlapping distributions, which can be illustrated as follows:

The vertical blue line represents the cutoff between positive and negative test results. In this illustration, the cutoff is placed in a compromise position between the two populations, creating a group of false negatives (FN) and false positives (FP).

If a test is highly sensitive, the cutoff is shifted to the left, eliminating false negative results, but increasing the number of false positive results.

If a test is highly specific, the cutoff is shifted to the right, eliminating false positive results, but increasing the number of false negatives. As we have discussed previously, this is the situation with antigen tests for SARS-CoV-2.
When screening large populations for disease, it is important not to miss possible positives, so we choose a test that highly sensitive. We do not want any false negatives. False positives can be sorted out later; this is just a screen after all. On the other hand, it is important that confirmatory tests have high specificity. When we are confirming disease in a population selected by a screen, we want to eliminate false positives.
If the goal of testing for SARS-CoV-2 is to avoid false negative results, favor sensitivity over specificity. But this trade-off is not necessary with all test systems. PCR tests increase sensitivity by amplification and increase specificity with detection probes unique to the virus. The result is a separation between populations, increasing specificity and sensitivity at the same time:

Are sensitivity and specificity the only considerations when evaluating a test? No, it is more complicated, but I am sure you guessed that. We will talk about other measures of test systems and the results they produce next time.
- Accuracy, Precision and Predictive Value
We want accurate tests, don’t we? By that, don’t we mean that we want precise test results? Well, not exactly. Before we leave the subject of laboratory statistics, there are a few more words we need to learn.
Accuracy is the ability of a test to aim for the target. Visually, accuracy looks like this:

Even though none of the shots hits the bullseye, we can tell where the shooter is aiming.
Precision is the ability of a test to get the same answer repeatedly, illustrated like this:

Even though none of the shots hits the bullseye, all of the shots go to the same spot.
Putting these terms together, we can describe different aspects test performance. Poor accuracy and poor precision look like this:

The shots are not centered on the bullseye, and they do not hit the same spot. Together, favorable accuracy and precision can be illustrated like this:

All the shots hit the bullseye, repeatedly. This is what an accurate and precise test looks like, too. Accuracy and precision are both desirable but different aspects of test systems.
But are accuracy, precision, sensitivity and specificity enough to interpret tests? Consider the case where these aspects of a test system are optimized. In other words, the test is highly accurate, precise, sensitive and specific. But what if the condition being tested for is not prevalent in the tested population. Prevalence is the percentage of people in a given population who have the condition of a positive test. Consider a test is 99.99% specific. That means that for every 10,000 results, there is only 1 false positive. But let’s say that the condition exists in the population at a rate of only 1 per 10,000 individuals. In other words, out of 10,000 results, there is only one true positive result. But we’ve already said that out of 10,000 tests, there will be one false positive result. Therefore, if we get a positive result, there a 50% chance it’s the false positive, not the true positive. That is what is meant by the term positive predictive value.
Both positive and negative predictive values can be measured. These are expressed mathematically as PPV = TP / (TP + FP) and NPV = TN / (TN + FN), respectively. It’s okay to skip the math; just remember that predictive values are dependent on the prevalence of the condition; sensitivity and specificity are not.
Predictive value is important for test interpretation but should not be used for test selection. Instead, sensitivity, specificity, accuracy and precision should be used to guide appropriate test selection. These are the terms by which test systems are judged, and the key aspects of test performance analyzed by the FDA before tests are approved for use in the United States.
- Quarantine
In guidance updated December 2, 2020, the CDC adjusted quarantine period for asymptomatic individuals. Today we consider these latest quarantine recommendations.
Before we do, we must first discuss what it means to quarantine and the conditions that trigger a quarantine. Quarantine separates an individual who may have been exposed to SARS-CoV-2, the virus that causes COVID-19, from others to prevent further spread of the virus. Simply stated, quarantine means stay home and stay away from others. If you live with other people, keep to a separate room. If you must be in the same room with someone else, stay 6 feet away, wear a mask and make sure everyone else does too. Generally, if one person in a household is quarantined, all persons in that household should also quarantine.
You must quarantine when (1) you have COVID-19, (2) you first positive test for SARS-CoV-2, or (3) you are exposed to someone infected by SARS-CoV-2. An exposure is an encounter of less than 6 feet apart and more than 15 minutes long when one or both individuals are not wearing face masks.
The standard quarantine period for asymptomatic individuals is 14 days. This recommendation comes from the maximum observed time between exposure and development of symptoms, known as the incubation period. The incubation period is less than 14 days for most infected individuals, with 5-7 days being average.
The new CDC guidance lists two situations when the quarantine period can be shortened to less than 14 days. If no symptoms develop, the quarantine can be ended after 10 days without testing for SARS-CoV-2. But if the person tests negatively for SARS-CoV-2 on or after the 5th day of quarantine, and if the person never develops symptoms, then the quarantine period can be ended after day 7. For the purposes of counting days, the exposure day is considered day 0.
Immediate testing at the time of exposure is not recommended. Testing prior to 5 days after exposure does not shorten the recommended quarantine period and could lead to a false perception that the exposure did not lead to infection, perhaps promoting risky behavior.
The quarantine period is different if you have symptoms. For persons with mild illness, the quarantine period is 10 days from the onset of symptoms or 24 hours since the last fever without use of fever-reducing medicines such as Tylenol, whichever is longer. Generally, a mild illness is one that does not require hospitalization. If hospitalization is required, the quarantine period may be 20 days or more, depending on the advice of your doctor.
Following these updated quarantine guidelines slows the spread of the disease and keeps your loved ones safe. However, wearing a mask and staying away from people who are not wearing masks minimizes the risk of exposure in everyday encounters. More on masks next time.
- Mask Up!
Individuals exposed to someone infected by SARS-CoV-2 should be quarantined to slow the spread of COVID-19 and keep our loved ones safe. However, being quarantined is a lot like being in jail. How can we avoid drawing this card?

We have learned a lot about the spread of SARS-CoV-2 in the last ten months. Those exposed to individuals infected by the virus are at risk of becoming infected themselves. According to the CDC, an exposure is an encounter of less than 6 feet apart and more than 15 minutes long when one or both individuals are not wearing face masks. By this definition, wearing a mask and keeping your distance from those not wearing masks prevents exposure to SARS-CoV-2.
Does that mean that you will never get SARS-CoV-2 if you wear a mask? No, wearing a mask cannot prevent all SARS-CoV-2 infections, but it will dramatically reduce your risk of infection and your risk of being dragged into quarantine jail.
How do we know that masks work? The CDC has published evidence for the effectiveness of masks. To this list, I add two observations from my own experience.
In the hospitals where I work, all physicians, staff, patients, and visitors are required to wear masks. Although some individuals have become infected with SARS-CoV-2 during the pandemic, contact tracing demonstrates that individuals were infected outside of work. I have not observed “hot-spots” of infection in clinical areas where these precautions are practiced. This, despite treatment of hundreds of patients with COVID-19 at these hospitals.
The second point is the absence of flu in Texas this December. By this time of the year, flu season is generally in full swing. In mid-December, the laboratories where I work have usually detected many positive flu samples. However, this year these same laboratories have yet to see their first positive flu test. This is not for lack of testing for flu. Since October, every rapid PCR test for SARS-CoV-2 has included a test for flu.
Why is this observation relevant? Flu is a respiratory illness transmitted in much the same way as SARS-CoV-2. What prevents spread of coronavirus also prevents the spread of influenza virus. With masking orders in place, the spread of flu has dramatically reduced.
If masking has effectively stopped the spread of flu, why is COVID-19 surging? Coronavirus is much more infectious than flu. The point is that masking reduces all disease that spread by the airborne route. Imagine what the surge would be like without masking?
In Texas, we love to wear our boots and hats. This year, we’ve learned to love our masks, worn all the way up, covering the nose and mouth. Be safe during the coming holidays. Mask up, y’all!
- Viral Variant
A new variant of the SARS-CoV-2 virus is emerging in Great Britain, becoming the dominate form of the virus that causes COVID-19 in London and southeast England. What are the implications of this new variant?
The new variant has been officially named “SARS-CoV-2 VOC 202012/01.” You may also see it referred to as “B.1.1.7”, or “SARS-CoV-2 Variant” in both the popular and scientific press. This variant has a mutation in one of the spike proteins which binds the virus to human cells during the infection process. So far, this variant has not been reported in the United States.
Viral mutations are common. In fact, many different strains of the SARS-CoV-2 virus are likely to exist in the United States right now. But so far, none of these mutations has caused a significant difference in the binding capacity of the virus to human cells. At least none that we know of. Our understanding of SARS-CoV-2 continues to evolve rapidly.
The variant identified in England seems to spread more quickly in humans. The thought is that the change in spike binding protein makes it more likely for the virus to stick to human cells.
Why does increased stickiness of virus affect the virus’ ability to spread? After the virus sticks to the cells lining the inside of the nose and upper airways, the virus injects its genetic material into the human cell. This genetic material is programmed to take over the machinery of the cell, causing it to abandon its usual functions and become a virus producing factory, spewing out hundreds of new copies of the virus. These new viral copies infect other cells, either in the same body, or in bodies nearby. This accounts for the waxing of disease within a sick, infected person, and the spread of virus from person-to-person. If the virus is stickier, more human cells are taken over, and more copies of the virus are produced, making it easier for the virus to go, well, viral!
Will tests detect this new virus strain? Yes, PCR tests will, at least for now. Because PCR tests use two or three different detection targets, the change in this variant’s genetic code is not enough to evade detection by PCR tests. However, as the genetic code of the virus continues to evolve, it is conceivable that a mutation will arise that is not detected by tests currently in use, even PCR tests. Antigen tests, which already have low sensitivity, do not share the multi-targeted feature of PCR tests; therefore, even more false negative antigen test results can be expected when the variant becomes more prevalent.
Will the variant reduce the effectiveness of vaccine? The honest answer is that we really don’t know. Theoretically, this variant will not, since the vaccines released in the U.S. are polyclonal, causing the formation of antibodies to several different parts of the virus’ spike proteins. The theory is that even if one part of the spike protein changes, the antibodies will still be effective against the other parts that have not changed. But theory and reality are not the same thing. We won’t know for sure until vaccine effectiveness has been studied in populations infected by the variant.
This brings us to one final point about this viral variant. This variant is undoubtedly the first of many variants to come, and the answers for these yet-to-be-seen variants may be different than the answers for this one. Viruses want to survive. Just as the use of antibiotics causes the emergence of antibiotic resistance in bacteria, the use of vaccine will favor viral mutations that evade vaccine-induced immunity. Variants will emerge that are unaffected by vaccine.
The pandemic is a war, both metaphorically and really. Our best defense is the practice of what we know reduces spread: mask up, keep apart, and isolate when exposed. We will prevail. But it’s still too early to celebrate victory.
- Spread and Detection of Variants
Last time we learned that a new strain of the SARS-CoV-2 virus has emerged in London and southeast England. This variant strain, called “VOC 202012/01” or “B.1.1.7” is more infectious than the standard SARS-CoV-2. It has quickly spread to other parts of Europe, and its presence is now reported in Canada and the United States. At least two other distinct variants are reported in South Africa and Nigeria. How do we keep track of these variants, and what does their rapid spread mean?
The variants are named by adding suffixes of letters and numbers to help keep the many cataloged mutations straight. Two different systems may be used. For example, the South African variant is labeled “501Y.V2”, but it is also known as “B.1.351”. The Nigerian variant is called as “B.1.207”. Neither of these has been labeled a “variant of concern”.
A “variant of concern” is a strain is associated with differing clinical features such as greater disease severity or faster spread. “Variants of concern” will have the letters “VOC” in their name. So far, the first and only “variant of concern” is VOC 202012/01, the variant identified in London which has now spread into Europe, Canada, and the United States.
While none of the variants identified so far seem to evade detection by the PCR tests generally available to the public, these tests will not tell you whether a detected virus is one of the variants. Specialized sequencing is required to identify a virus as a variant. This testing is conducted on a regular but limited basis by the CDC, state and local health departments, and various universities.
The CDC is watching the evolution of variants closely. The concern is that increasing numbers of variants may change the way the virus spreads, may reduce detection by current tests, may create resistance to drugs such as monoclonal antibodies, or may produce a strain that evades immunity caused by vaccine or previous infection. We will watch too. As the “variant of concern” spreads into the United States, remember what keeps us safe: mask up, keep apart, and isolate when exposed.


{kind=link}