The American Medical Association (AMA) urges physicians to promote COVID-19 vaccines and bivalent boosters. The AMA even supplies members with social media talking points and strategies to deal with vaccine detractors. It is not the first time that my profession has endorsed a product that may be hazardous to your health.

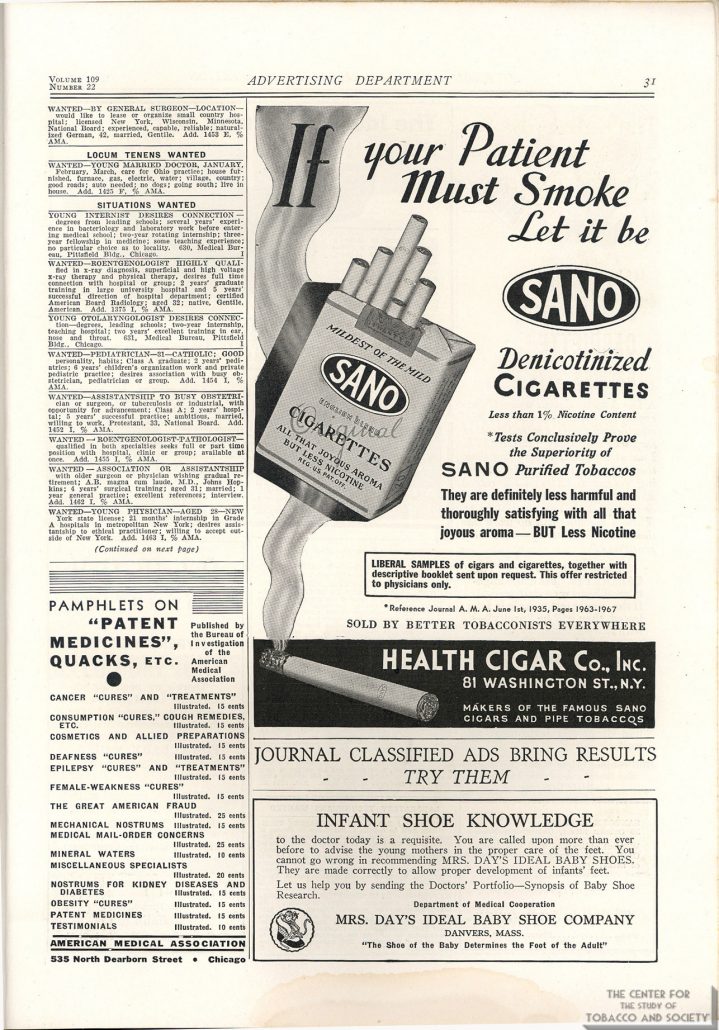
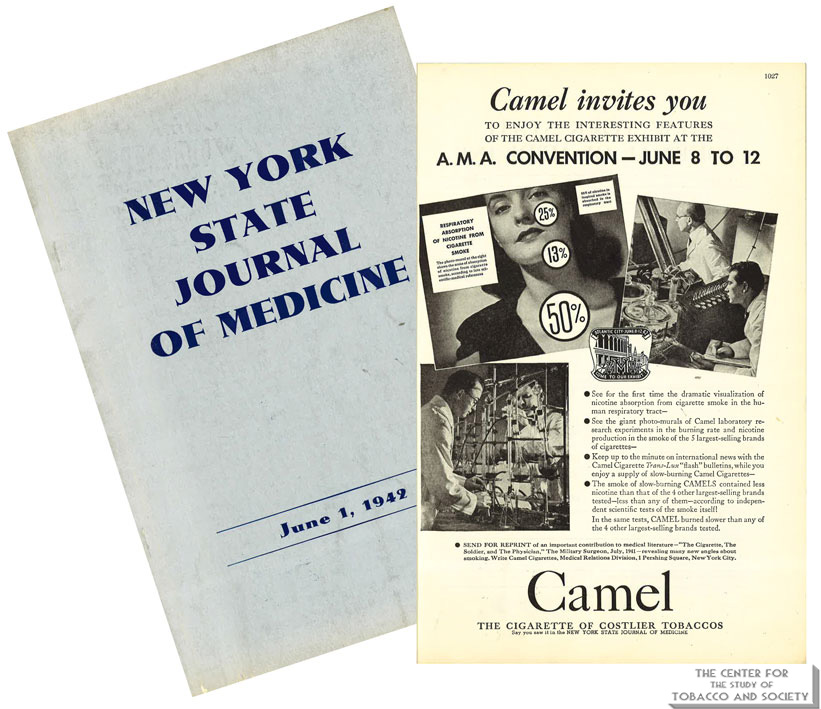
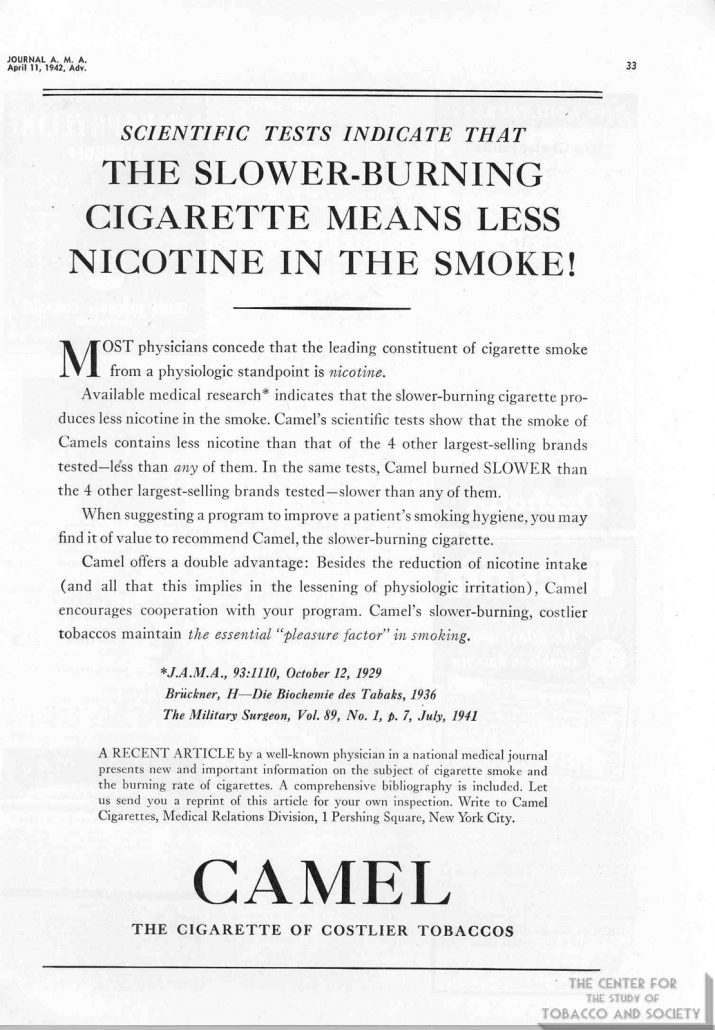
For most of the twentieth century, the AMA turned a blind eye toward the dangers of tobacco use. During the 1930s, 40s and 50s, tobacco companies paid handsomely to advertise cigarettes in AMA’s journal, JAMA. In a 1948 editorial minimizing the ill effects of smoking and justifying tobacco advertising in its publications, JAMA noted that “cigarette business is a tremendous business,” as if the size of the bottom line can mitigate a conflict for an organization founded for the “betterment of public health.”
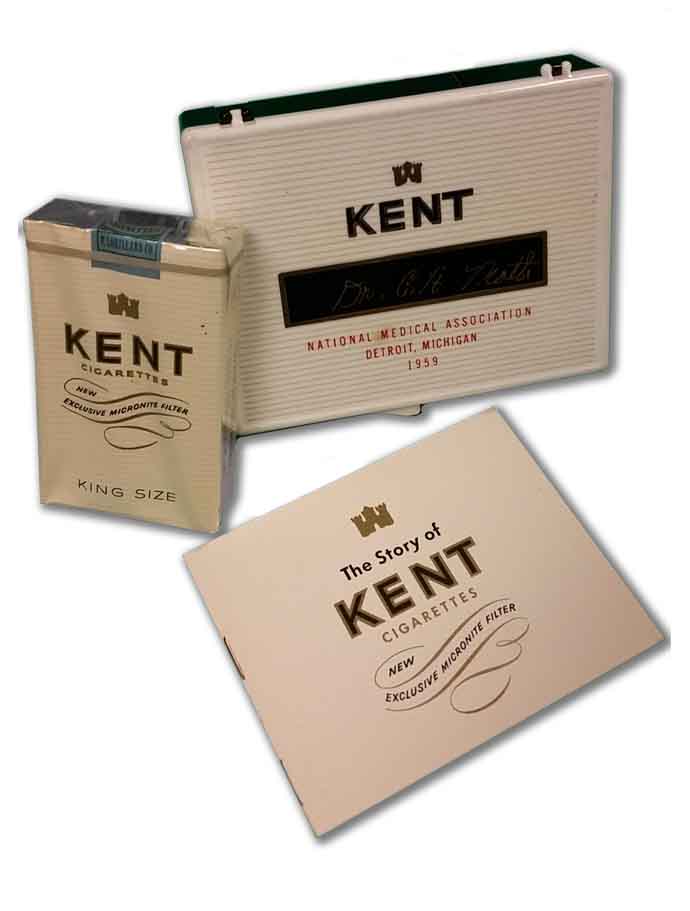
The connection between smoking and lung cancer was recognized early in the century. At the same time, the AMA became increasingly dependent on money generated by tobacco sales. Tobacco companies sponsored meetings of medical societies, setting up their booths alongside exhibitions of the latest medical treatments. Free cartons were distributed at physician meetings. Cigarette makers even paid for publication of pseudoscientific reports claiming the health benefits of their products.

Doctors who opposed smoking faced ridicule from their colleagues. Dr. Alton Ochsner, a renowned surgeon and sentinel voice warning of the dangers of tobacco, began publishing on the connection between smoking and lung cancer in the early 1940s. His 1954 book Smoking and Cancer: A Doctor’s Report was negatively reviewed in prominent medical journals, characterized as a medieval model of logic that belongs in the nonscience section of a library. Prior to his appearance on Meet the Press, Dr. Ochsner was told he could not discuss the relationship between smoking and lung cancer on air.
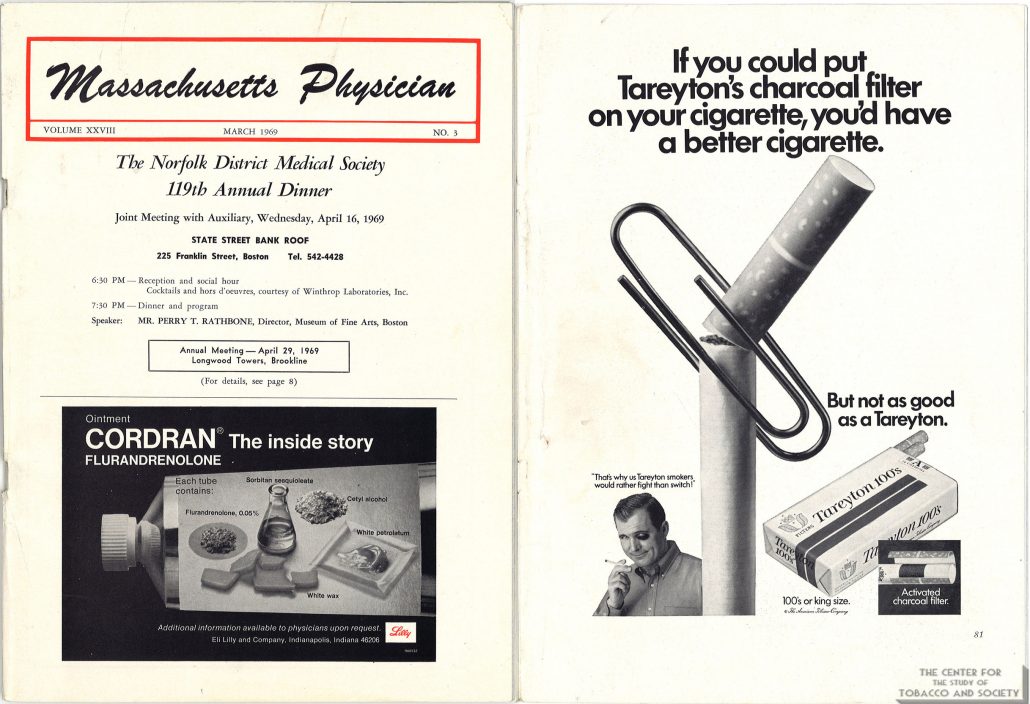
Yet the mounting evidence was hard to ignore. In 1954, JAMA stopped accepting cigarette advertisements and published an editorial rebuking tobacco company advertising practices. But fives years later, a JAMA editorial was still skeptical of the evidence linking smoking to cancer, and a 1961 Nebraska State Medical Journal editorial dismissed the evidence as merely “statistical.” Tobacco companies continued to sponsor state medical meetings as late as 1969. By then most people were aware of the dangers of smoking.
In 1964, the Surgeon General concluded that cigarette smoking causes lung cancer and other life-limiting health conditions. The next year, a warning label was required on packages of cigarettes. By 1971, the government banned cigarette advertisements on television and radio. Instead of taking the lead against an obvious threat to public health, the AMA asked for time and money to study the effects of tobacco.

Between 1964 and 1976, the AMA received more than $20 million from the tobacco industry to fund research. Instead of using the money for smoking cessation programs, many of the funded studies focused on ways to make a safer cigarette. To keep money flowing into its Education and Research Foundation the AMA delayed, stating in a confidential 1971 report that, “AMA is not prepared to make any statement regarding termination of the smoking-health research program.” The report went on to complain that tobacco companies are “in arrears on 1970 contributions.” The dependency on tobacco money created a political alliance between doctors and cigarette makers as their lobbyists joined forces in Washington.
The delay benefitted tobacco sales and maintained the AMA’s “research” payments, but it angered Dr. Ochsner, who accused the AMA of being derelict. The AMA called Dr. Ochsner’s position “extreme.” However, name-calling could not stall the inevitable conclusion any longer. In 1978 the AMA finally agreed with what most people had already realized: smoking causes lung cancer, and many other health problems. The romance with big tobacco was over.
Or was it?
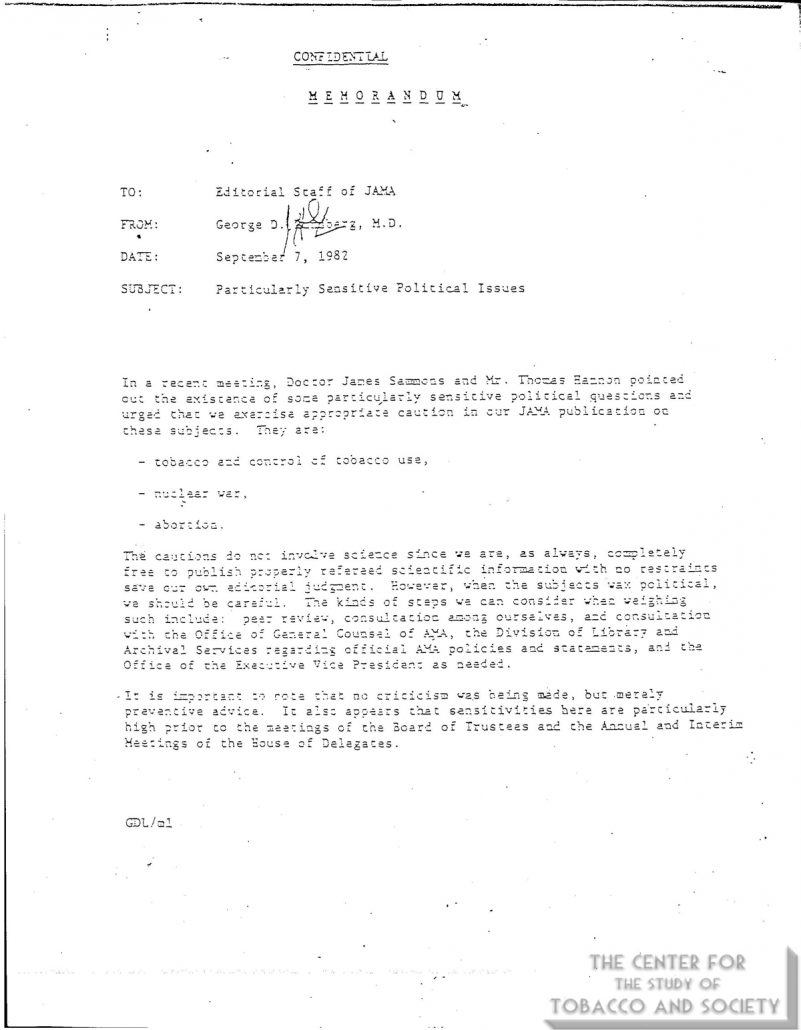
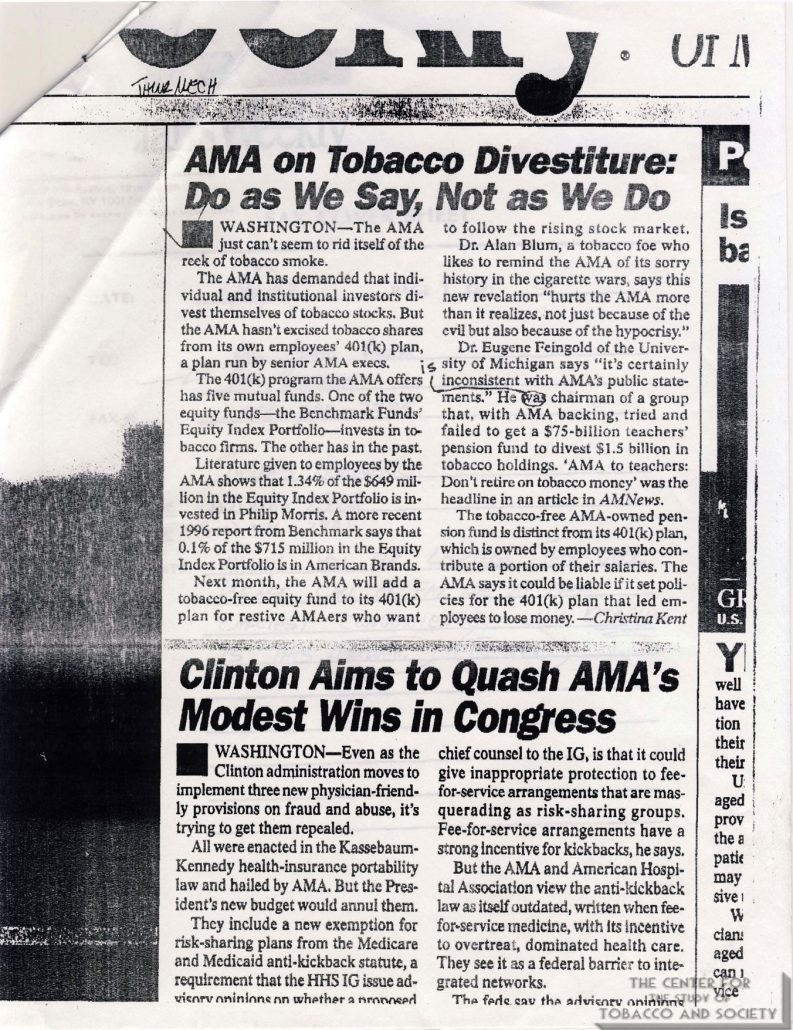
As late as 1982, JAMA publications were warned to steer clear of “politically sensitive” topics like tobacco use. After most of a century of being on the tobacco dole, the AMA could not make a clean break. The AMA portfolio contained investments in tobacco companies until the late 1990s.
In 1998, the tobacco industry settled lawsuits filed by state governments with a massive Master Settlement Agreement. In exchange for perpetual annual payments and tight regulatory control, the tobacco industry could continue to sell its products protected from future lawsuits brought by participating states and jurisdictions.
But who really benefitted from the Tobacco Settlement? Only 2.6% of the money has been used for smoking prevention and cessation programs. Some states have used the tobacco money to fill budget gaps. South Carolina gave money to tobacco farmers affected by a drop in prices. Altria Group, a global tobacco company, is on the US News 10 best-performing stocks list. Altria, Phillip Morris, and British American Tobacco have all grown annual dividends consecutively since the settlement. According to Dr. Ed Anselm, “The most addictive thing about tobacco is money.”
Tobacco use remains the number one preventable cause of death in the United States. In the first fifty years after the Surgeon General’s 1964 report, more than 20 million Americans died of smoking. How many of these deaths would have been prevented if doctors had not been conflicted by financial entanglements with the tobacco industry?
Money blinds objectivity. When money drives decisions, controverting evidence is ignored, dissenting voices are ridiculed, open debate is suppressed, talking points are distributed, conclusions are delayed, and people die from a product with liability protection.

The New York State Journal of Medicine published a retrospective of tobacco’s relationship to medicine in its December 1983 issue. Flipping through the pages is enlightening. Surrounding the articles describing the greed and politics of big tobacco are advertisements from medicine’s new love—big pharma. Doctors have exchanged one bedfellow for another.
By endorsing irrelevant COVID-19 vaccines and poorly tested bivalent boosters, the AMA is pushing a product without concern for its potential negative health effects. Like before, the medical profession lags behind public opinion. According to recent Rassumsen Reports, 7% of vaccinated individuals report a major side effect, and nearly half of Americans believe that COVID-19 vaccines have caused unexplained deaths, about the same proportion who believed that smoking caused cancer in the 1960s while the AMA was studying the issue.
A conflicted profession cannot honestly evaluate data. Nowadays, the pharmaceutical business is a tremendous business. An organization benefitting from a product’s sales cannot be trusted to evaluate that product.
If doctors could not recognize the health dangers of tobacco for most of the last century, why should we believe them when they say novel vaccines are safe and effective?
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}